
ANAL FISSURE
Dr Arun Prasad, MS, FRCS, FRCSEd
Senior Consultant Surgeon Minimal Access Surgery
Apollo Hospital, New Delhi, India
Email: surgerytimes@gmail.com
Tel: ++91-11-29871202
Contents ( Please click )
WHICH DISEASE ??
| BLEEDING | PAIN | DISCHARGE | CLICK BELOW | |
| PILES / HEMORRHOIDS | ++++ | + | + | piles |
| ANAL FISSURE | ++ | ++++ | + | fissure |
| ANAL FISTULA | + | ++ | ++++ | fistula |
Please select from the above table, the most appropriate disease you may be looking for. The above is a rough guideline and needs to be confirmed with local examination by a specialist doctor.
Piles in India is generally used as a loose common term to include piles, hemorrhoids, fistulas and fissures with skin tags.
Fistulas are an abnormal small opening next to the anus from where discharge keeps occurring. This is due to a tunnel like tract between the anal canal and the skin. This condition always requires surgery for cure.
True piles are those that present with PAINLESS BLEEDING due to swelling up of blood vessels in the anal canal.
Fissure with skin tags lead to painful bleeding due to a small cut at the anal margin. It is usually associated with skin tags that are mistakenly called piles. This condition resolves in majority of the patients by use of creams and medicines to treat constipation. Skin tags can sometimes be a source of great irritation due to micro-incontinence. Rarely the patient needs surgery.
ANAL FISSURE DETAILS
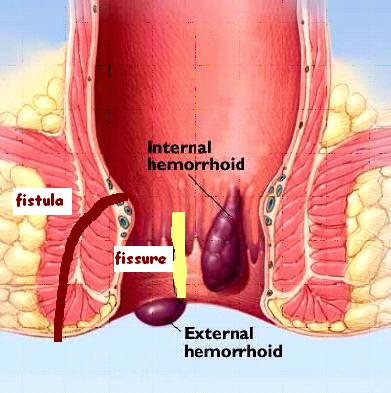
A fissure consists of a crack or tear in the vertical axis of the inner lining of the anal canal just above the anal verge.
Initially it is superficial but may deepen to reach the underlying muscle fibers.
Fissures usually occur in the posterior midline.
Fissures are often associated with secondary changes which may include a skin tag (also known as a sentinel pile though it is not actually ‘piles’), hypertrophied anal papilla, and relative anal stenosis secondary to spasm of the muscle sphincter.
Anal fissure is a common
and minor disorder but merits careful attention because it is painful and the
treatment is simple and effective.
It has been proved beyond doubt that constipation is the basic and sole cause of
initiation of a fissure. During the passage of hard stool, the posterior midline
area of the anal canal which is rather poorly supported, so the connective
tissue tends to get excessively stretched and may get abraded at places. The
abrasion recurs and recurs and is converted into a frank longitudinal tear in
the sensitive anal lining, the true fissure in ano.
A fissure may arise from
1. Trauma to the anus (constipation is the most common cause, surgery, injection, rubber banding, sigmoidoscopy, colonoscopy, etc.),
2. Rarely, it may be a manifestation of a specific underlying disease state such as chlamydia, gonorrhea, herpes, syphilis, AIDS, tuberculosis, cancer, Crohn's disease, or ulcerative colitis.
Pain:
Sharp agonising pain starts when the individual passes stool. The pain is severe. Persist for an hour or more. It ceases suddenly. The sufferer is comfortable until the next action of bowel. The individual tends to be constipated rather than go through painful ordeal.
Bleeding
Small amount of bright red blood streaked on the stool.
Skin tag
A small skin tag may form at the lower end of fissure, which the patient can feel.
The symptoms are slow to develop and long lasting. They hardly ever disappear spontaneously. But many people suffer for months before going to see their Doctor.
The diagnosis can be made by inspection, palpation, and/or Proctoscopic examination by a Specialist Doctor.
The best way to prevent fissure is to keep stools soft so they pass easily, thus decreasing pressure and straining, and to empty bowels as soon as possible after the urge occurs. Increased fibre in the diet helps reduce constipation and straining by producing stools that are softer and easier to pass. If the diet cannot be modified in this way, adding bulk laxatives may be necessary; they can prevent worsening of the condition.
Most of
us have encountered an episode of burning anal pain during defecation once in a
while. This is the stage of abrasion of the anal mucosa. But how many of us have
really sought any medical treatment for it? The answer will be no in most cases.
Because the episode is so trivial that very next day everything seems to settle
and this holds true with the common masses also.
Most of the casual attacks of anal pain are either neglected or are treated by
the family physicians with various preparatory creams and laxatives.
We can call these fissures as simple or superficial. It has long been recognized that simple fissures can be cured conservatively.
In addition, a person should not sit on the toilet for a long period of time.
MEDICAL TREATMENT
Most of us have
encountered an episode of burning anal pain during defecation once in a while.
This is the stage of abrasion of the anal mucosa. But how many of us have really
sought any medical treatment for it? The answer will be no in most cases.
Because the episode is so trivial that very next day everything seems to settle
and this holds true with the common masses also.
Most of the casual attacks of anal pain are either neglected or are treated by
the family physicians with various preparatory creams and laxatives.
We can call these fissures as simple or superficial. It has long been recognized that simple fissures can be cured conservatively.
1.
A non-constipating diet, and a warm Sitz bath gives a fair amount
of relief and a virtually painless defecation.
2. Topical creams deserves a special mention as they are being
used very often and do provide a good amount of amelioration of symptoms plus a
Psychological satisfaction of doing a ‘local’ therapy for a localized pathology.
Ointments containing opiates, xylocain, amethocain and cinchocain to relieve
pain, Belladona to alleviate sphincter spasm and silver nitrate to promote
healing have been advocated since long. The mixture was introduced on the finger
or a short nozzle to ensure its application to the inner part of the fissure.
3.
Local application of vasodilators— Nitric oxide donors such as glyceril
trinitrate [GTN] or isosorbid Di nitrate cause a chemical sphincterotomy leading
to healing of fissure.
A GTN ointment applied twice for 6 weeks gave complete healing in 98% of
patients. Successful treatment may come at the expense of a high incidence of
headaches and a lower compliance. A balance is required between fissure healing
and headache intolerance.
Diltiazem and Nifedipine creams / ointment / jelly are now available and do not have the side effect of headaches. These have become very popular of late. The only problem with local medications is the difficulty in applying it at the correct place.
Some studies have also reported a high incidence of recurrence.
But during the course of therapy strict dietary restrictions to smoothen the stool are utmost necessary. Similarly the long-term affectivity of the therapy is not well documented.
4.
Injection of Botulin Toxin- Known to cause paresis of the sphincter and
thus 2.5 to 5 units of Botox is injected bilaterally to the fissure. This causes
sphincter paresis for about 3 months, a time enough for healing of a chronic
non-complicated fissure.
It is well tolerated and can be administered on an outpatient basis. The healing
rate reported is about 79%.
The toxicity of the drug, accidental injection in the surrounding tissue,
haematoma and infection has discouraged its regular use and practice.
The fissure is labeled
as complicated in the following situations:
1. Not responding to conservative treatment.
2. Association with anal polyp.
3. Presence of an external skin tag (sentinel pile).
4. Presence of hemorrhoids or a fistula underneath.
5. Thick edges of fissure.
6. Exposure of the muscle fibers at the floor of the fissure.
7. Infection at the base of fissure.
It has been shown that fissure complicated by any of these facts will not heal spontaneously and will not respond to conservative therapy.
1. Stretching of anal
sphincter- this is one of the most
favorite method of treating the anal fissures. The great attraction of the
procedure is due to its extreme simplicity and need of almost no instrument and
thus performance at the most remote and unequipped hospital even by a junior
staff.
The mechanism by which anal dilatation cures anal fissures are by reducing the
anal canal pressure.
2. Fissurectomy (Excision of the anal fissure ). Here a triangular
part of the tissue is excised along with the fissure itself. This procedure is
usually preceded by anal stretch.
Although, a very good and reliable operation, it leaves behind a large and
rather uncomfortable external wound which takes a long while to heal.
3. Sphincterotomy
(Division of internal anal
sphincter)- This is today’s most preferred therapy for chronic and non-healing
fissures.
This can be done by two ways:
a. Pharmacological (as described above)
b. Surgical under general anesthesia. A small internal cut is made which divides
the muscle fibers which have been causing the spasm and not allowing the fissure
to heal. The divided fibers along with the fissure would heal on its own in
about 2 weeks. This procedure known as Lateral Internal Sphincterotomy is
regarded worldwide as the most successful method of treating a fissure.
A lot has been talked about Laser Surgery. This as opposed to conventional scalpel and electrocautery techniques, is associated with many myths. Many doctors and quacks have touted painless or decreased pain and shortened healing times as advantages to performing surgery in this area by laser. No documented studies support these claims. In fact, most studies across the world have shown that Laser piles surgery has no advantages over standard techniques; it is also quite expensive and no less painful.
A consultation with a specialist doctor including a proctoscopic examination would cost between Rs 900 to Rs 1500. Medical treatment for 2 weeks would cost around Rs 500. Surgery if needed could cost between Rs 20,000 to 40,000 depending on the hospital / clinic.
The author Dr Arun Prasad MS, FRCS is a senior Gastro-Intestinal and laparoscopic surgeon at Apollo Hospital, New Delhi. He has been trained in Proctology Surgery at the prestigious Charing Cross Hospital in London after qualifying for the FRCS. He is one of the first surgeons in India to have started the Stapled Hemorrhoidectomy procedure and is a trainer in India for same.
PHONE
91-11-29871202
