
![]()
![]()
![]()
![]()
KARL MAY AND JUSTICE JUSTICE FOR KARL MAY.
Two articles appeared recently in the 'Jahrbuch der Karl May Gesellschaft.'[1] [2]
The authors of both publications present Karl May from a negative viewpoint.
They also question the concept of Dissociative Identity Disorder (D.I.D.).
Author of the 'Karl May and Justice' is of an opinion "that May now more knowingly and willingly acted, for which speaks the careful planning and the cool appearance"[3] during the period of 1862-1870, when he was apprehended by the authorities. The article also assumes "He [i.e. Karl May] acknowledged his fraudulent role, therefore was always aware of it."[4] Another opinion is offered: "As a multiple personality this could have never and never occurred to him."[5] And once more some researchers speculate: "In a semiconscious state May would not have been able to carry out his criminal offences."[6]
In a previous publication[7] I have described the state of mind Karl May found himself during the years 1862 till 1874. It is called the Dissociative Identity Disorder (D.I.D.). This is a complex disorder that has only recently been fully recognized. Most Psychiatric and Psychological Associations recognize the diagnosis, as well as the Index Medicus, the world largest and most universally accepted database of clinical articles published by journals and accepted as scientifically valid. The complexity of this disorder is still causing disbelieve, confusion and on occasions questioning by some psychologist or even psychiatrists.
However an outright rejection of D.I.D. as the authors of (1) and (2) do is not warranted. This is of importance because either Karl May was a criminal in his youth, or there is a different explanation for his behaviour during 1862-1874, which was so out of character with the rest of his life.
There appears to be confusion in the minds of the critics with regard to Karl May and D.I.D.
Firstly they labour under the impression which the popular press, television programs, movies and various dubious personalities managed to present to the public.
Secondly they confuse the Dissociative Disorders group with Multiple Personality Disorder (M.P.D.), not noticing the difference in classification in the 'Diagnostic Criteria from DSM-IV'[8] and the 'ICD-10-CM'.[9]
Thirdly there is in their minds an idea that a patient with D.I.D. (or as they refer to this as M.P.D.) is acting in a hazy somnambulist state, like a zombie, not remembering anything, out of touch with reality.[10]
Fourthly there is another statement in (1) which is clearly not true: "that in the modern forensic psychiatry the diagnosis of multiple personalities will be considered as an iatrogenic artefact."[11] 'Iatrogenic' in medical terms means an illness or symptoms induced in a patient as the result of a physicians words or action. Patients come to medical doctors with clear cut symptoms of D.I.D. to seek treatment, and not vice versa.
Fifthly over the years Karl May had been named at different times a personality with schizoid, histrionic, narcissistic disorder, and lately even declared a life long case of bipolar disorder. Somehow it became a tradition to stereotype May as a criminal, vagrant, Hochstapler [confidence trickster], mentally insane and generally of no good character.
(A). An opinion is expressed in (1) speculating that if Karl May acted before 1870 in a "hazy", "semiconscious" state of mind ["Dämmerzustand"], he would not have been capable of deeds he was accused of. From this the author of (1) deduced that May could not have suffered from D.I.D. Such supposition of course has not been confirmed by the current clinical knowledge of D.I.D. As already mentioned see reference (10) the 'dream like' condition applies only to one of the Dissociative Disorders, the Depersonalisation disorder, and not to the whole group. When the criterion B of D.I.D. is applied it does not mean the patient has to act in an irrational way because of dysfunction of mental ability. It is well known from clinical practice that D.I.D. patients do not act in some "hazy dozy state of mind", but act as fully functional, rational and logical alter personalities.
It is important to know that reality testing remains intact in patients affected by dissociative disorders.
It is of great interest to note in this connection that Karl May mentioned this long before the fact has been confirmed by clinical tests: "I was sick in my soul, but not in my mind. I had the capability to reach logical conclusions, to solve every mathematical problem."[12]
None of the required conditions of D.I.D. implicate that memories or behaviour of the alters have to be repressed, irrational, hazy or semiconscious [except D].
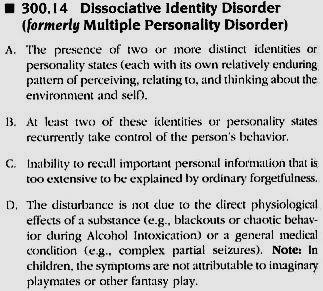 |
Criteria for DID from An imaginary "dozy state" or "semiconscious state" [Dämmerzustand], as some researchers presume Karl May had to be in, is not correct.
|
(B). The other opinion in (1) is that Karl May did not suffer from D.I.D., because he fully confessed, the hypothesis being that Karl May must have been aware of what he had done.
In fact because[13] "He [i.e. Karl May] acknowledged his fraudulent role," does not mean "therefore [he] was always aware of it."
Repressed or recovered memories are not an essential part of the diagnosis of D.I.D. Many patients have very good recollection of what happened to them in their childhood, as well as of court transcripts, external corroboration, and other witnesses. Karl May may have been told, or may have read what he was accused of. Because May 'acknowledged' his behaviour does not mean he was 'always aware of it.' According to the latest medical view[14] in dissociative identity disorder some of a persons personalities are aware of important personal information, whereas other personalities are unaware. Some personalities appear to know and interact with one another in an elaborate inner world. For example, person A may be aware of personality B and know what B does, as if observing Bs behaviour; personality B may or may not be aware of personality A. Other personalities may or may not be aware of personality B, and personality B may or may not be aware of them.
The switching of personalities and the lack of awareness of ones behaviour in the other personalities often makes life chaotic for people with dissociative identity disorder. Because the personalities often interact with each other, people with dissociative personality disorder report hearing inner conversations and the voices of other personalities commenting on their behaviour or addressing them. They experience distortion of time, with time lapses and amnesia. They have feelings of detachment from ones self (depersonalisation) and feelings that ones surroundings are unreal (derealization). People with D.I.D. may not be able to recall things they have done or account for changes in their behaviour.
There is as well another explanation.[15] Had May mentioned the hallucinations and his state of mind to the court, he could have been confined to a mental asylum.
From all the circumstances, observations by other people of Karl May, and from what is known today of signs and symptoms of D.I.D., it seems apparent that May suffered during the years 1862 and 1874 from a group of Dissociative Disorders. May described the D.I.D. not only in his biography, but already in 1888.[16] May also described Dissociative Amnesia, but most importantly the Dissociative Fugue, which had not been referred to in the textbook on Psychiatry.[17] May might have consulted this textbook in 1910 in order to clarify and understand what happened to him in the past.
![]()
Because one of the critiques by the good people who took the trouble to read my paper[18] was that mainly Karl Mays own writings have been used in the study (even if this is an accepted standard research technique), let us mention some other relevant facts, important for the diagnosis of D.I.D.
Items of unknown clothing found in personal possession. D.I.D. is a complex condition which has many variations along the scale between mild and severe cases. One symptom however has been consistently reported from all over the world, i.e. possession of, to the patient unknown, pieces of clothing in his/her wardrobe. This fact has even become a joke: "The wardrobe always provides a multiple choice of new clothing."
Dr. Kathrin Dornbusch from the Department of Clinical Psychology at the Friedrich-Schiller University in Jena conducted a research on D.I.D,[19] where one of the questions was: "Have you ever found in your wardrobe clothing and you could not remember buying this?"
Mays description of acquiring fur-coats he had no need for, and the corresponding Police reports, fall into this category.
Observations of Mays abnormal behaviour by other people. When arrested on 26th March, 1865, Karl May was observed as being "quite without movements and seemingly lifeless, and also, after the Police doctor was called in, [May] did not talk."The fact that a doctor had been asked to come and see May suggests an abnormal conduct.
A warrant issued by the authorities on 31st July, 1869, specified an interesting detail on May: " he speaks slowly, in selected phrases. Distorting his mouth when talking."
Lawyers Haase observation. The duty lawyer who was supposed to defend May, made this observation of the accused in May 1870: "The whole personality of the defendant made an impression at the main hearing of an odd person, who to a certain extent seemed to sit on the accused bench full of high spirits."[20]
Today a forensic psychiatrist would be asked for an opinion, as the reaction was quite inappropriate in the given circumstances. Haase used the word "komisch", meaning funny, comical, strange, or odd. It could also mean queer, peculiar, or even crazy. All these words refer to behaviour, appearance of people considered out of the ordinary, strange or unusual. Why was May behaving in such way is open to speculation. The fact is that he was not acting in a normal way as judged by others.
Dissociative Amnesia and Dissociative Fugue. May has been searching for explanation of his amnesia and hallucinations in a textbook on psychiatric diseases.[21] What is important is that May described a symptom which is not in the Griesingers textbook the Dissociative Fugue! The sudden, unexpected travel away from home or ones customary place of work, with inability to recall ones past, confusion about personal identity or assumption of a new identity, partial or complete.
Not only had May described the Dissociative Fugue in his autobiography, but he also wrote a story (first published 18881889) 'The Scout', in which William Ohlert represents his alter ego. This story is a description of D.I.D. symptoms, well before the time anyone ever heard of it.
The power of creativity in the healing process of D.I.D. Outlet to emotions through art, writing, music, dance, poetry, has been documented as very important in the recover. Today we have many such works created by D.I.D. sufferers.
In this context we find there is a surprising similarity if we compare the Karl Mays poem "Night Terrors", which could have been written as early as 1863, with poems composed by D.I.D. patients recently.
NIGHT TERRORS.
By Karl May.Do you know the Night, descending on Earth,
With hollow wind and heavy deluge;
Thick Night, through which star shine is given no berth,
No eyes see through the weathers dense wall?
Even if this Night is gloom, in morning there is refuge;
O lie down in rest and sleep without fear!Do you know the Night, descending on Life,
When Death tracks you down in your last camp;
The call of eternity sounding close by,
And fear stops still your hearts pulsing call?
Even if this Night is gloom, in morning there is a refuge;
O lie down in rest and sleep without fear!Do you know the Night descending on your Mind,
Which cries in vain, Salvation!
Nights serpent slithers into memory
And a thousand demons spit in your brain?
O keep away in sleepless consternation,
Because this is The Night that has no morning!
I AM ALONE AND LONELY.
By Dawn.I am Alone and Lonely
My home is a house of many
Yet, I am alone, lonely, and brokenEyes that can not see
Thoughts that have no home
Moving rapidly, yet remaining where I began
Alone, lonely, and breaking.Breathing, not breathing
No feeling, reaching to touch without moving
Being touched and not wanting to feel.
Is it real, is it real.
SHADOWLAND.
By Jeffrey.I am here
I think, I breathe, I feel and then
Darkness
I am here
I play and sing and write and dance and then
Darkness
I can hear them
I can feel them
Sometimes I can even smell them
But I cant speak outside, only here
And the voices echo off the walls of my mind,
Separated by dividers,
Like little cubicles and then
Darkness
I am.
CONFINED.
By DKZAs we sit here within our chamber,
We perceive our life, its short remainder.
We shall cautiously go out into that stead,
Where hate and deceit all make their bed.Wed much rather stay here and banish all thoughts
Of being on the outside like wool on the moths.
But then all the pleasures of life and of time
Cannot become a reality, not while were confined.We must when we exit out into the stormy cold,
Keep ourselves bundled up, appearing to be bold.
Well gaze back behind us to see what is left,
Knowing in the future there may only be death.A death not of body, of spirit or soul,
A death of the mind, so cruel and so cold.
Hopefully before we go, well be able to empty our minds
Of all the battles and tapes that have us confined.
Criterion C of DID: Inability to recall important personal information that is too extensive to be explained by ordinary forgetfulness. Karl May at the start of his prison term (14th June, 1865) was sent, as a former teacher, to perform clerical duties. He was found by the superiors unable to do so, and had to be reassigned to simple manual task.
In his biography[22] May described the affair: I was detailed into an office. I failed as a clerk to such an extent, that I was found useless. This was striking. They concluded that I must have been in a totally strange state of mind, as I had to know how to write!
The Albin Wadenbach incident Recognition of Alter Personalities. Nowadays in diagnosing the alter personalities the following procedures are taken: (1) Polaroid or digital camera picture is taken when an alter personality is out. (2) Tape recording of conversation between the therapist and alter personality is made. (3) When the patient is able to do his/her own writing, this proof may be convincing, since the therapist did nothing to put those words on paper.
Often there is resistance in the patient against accepting the diagnosis of D.I.D., since denial and repression are their favourite defence mechanisms. But when the therapist has adequate proof of amnesia spells in which alter-personalities make themselves known, this ought to be presented to the patient.
Karl May was Albin Wadenbach in January 1870, when apprehended by authorities. He wrote a letter "home" to the isle of Martinique in West Indies, described his property in America and the education he received there. Such a unique document if preserved would contribute much to the Mays story. In the overall concept of things and other signs and symptoms of D.I.D., this written record of Mays alter-personality would be priceless.
![]()
"After serving his prison term, May also abandoned his criminal career" claims the (1) article.[23] Of course, because May was cured from his D.I.D. And it was not a "criminal career", as May recognized himself, when he wrote: "What I did then would be in the present, more enlightened time heard not by a judge, but by a physician."[24]
Most of the rest of Mays experience with the Court of Law concerned defending his interest. May had to fight character assassination attempts, stealing of his writings and denying payment due to him, as well as unsubstantiated press attacks against him.
An example of this is Lebius publication of imaginary stories about Karl May, based on lies by a Richard Krügel, gardening hand from the place of Mays birth town.
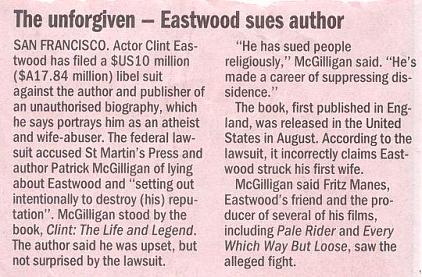 |
Times have not changed since, as the case of the film actor Clint Eastwood demonstrates.[25] |
This is not the right place here to discuss the "Diagnostic and Statistical Manual of Mental Disorders" [DSM]. The next fifth edition should appear around the year 2010. There is no doubt that under the pressure of various activists certain conditions are being either added or removed from classification of mental disturbances, as for example Post-Traumatic Stress Disorder (added) or Homosexuality (removed).
The inappropriate term Identity Disorder has been already removed from describing behaviour pattern during adolescence. "Multiple Personality Disorder" is no longer used for certain conditions as for example histrionic, attention seeking behaviour in adults. New controversies are being debated if pathological gambling is a disease, why not compulsive shopping?
Regardless of how common or rare a condition is, people have it. D.I.D. is a real complex condition and the clinical diagnosis is based on signs and symptoms which the patients demonstrate world over again and again. However the criteria are based largely on the presence or absence of certain behaviours, assessment of which could be subjective. Associate symptoms and behaviour can range in severity and occur in different combinations. Even if these days the most widely used diagnostic reference is the DSM-IV, some professionals also refer to the ICD-10, which provides a similar diagnostic perspective. Problem with terminology used is not well defined and can mean different things to different practitioners. There are different definitions given different systems.
In a situation like this, an experienced therapist, dealing with D.I.D. and not a lawyer should explain why the signs and symptoms as described above, would not be applicable to the diagnosis of D.I.D. in Karl Mays case during the period of 18621874?
OTTO RUBNERS ARTICLE.[26]
There are three points the author had tried to put forward:
None of the three conclusions are acceptable in view of the current medical thinking.
It is regrettable that Rubners diagnosis of Karl Mays state of mind did not extend beyond the conversion neurosis.[27] The old concept of neurosis in psychiatric classification has nowadays been replaced by three new categories: (1) anxiety, (2) somatoform, and (3) dissociative disorders. Formerly they have all been grouped together in the diagnostic category of neurosis. Rubner does not seem to be aware of this.
The Rubners old-fashioned term conversion neurosis, formerly called hysterical neurosis, conversion type, is today classified as somatoform disorder. The serious physical ailments of conversion disorder blindness, deafness, mutism, seizures, tics, anaesthesias, motor paralysis suggest neurological diseases but have no demonstrable organic or physiological base and are assumed to be an expression of psychological conflict or need. The incidence of these disorders appears to be declining in our times. Rubner missed this point that the past somatoform disorders have mostly changed in clinical presentation today into dissociative disorders.
The dissociative disorders, which are becoming more common,[28] involve some temporary change in consciousness, such as loss of memory for the past. In psychogenic amnesia there is the sudden inability to recall significant personal information accompanied by severe memory failure. Such memory loss is not caused by organic factors or simple forgetting. When the reaction does occur, it is often an object of attention in the media because of its intense, dramatic quality. The psychogenic fugue, the sudden travel away from home with loss of memory of previous life, belongs into this category.
The criteria for dissociative identity disorder have been described elsewhere and were included into the Diagnostic and Statistical manual[29] in 1994. Rubner stated in his article that he never ever in forty years of practice saw such a combination of symptoms.[30] This may have been so because Rubner did not take in the modern trends in psychiatry past the old concept of neurosis, and he never assessed the symptoms of a patient with dissociative disorder beyond the old fashioned conversion neurosis (hysterics).
Dissociative disorders occur cross-culture. In Germany a study group has been founded in 1995, with Dr.Ursula Gast, M.D., Psychiatrist, as a co-founder, at the Hannover University. There is a German w-page: http://www.dissoc.de as well as publications in medical journals.[31] [32]
Symptoms of dissociation have been described already in 1956 in
a standard textbook of psychiatry in central Europe[33]
and Rubner could have come across similar in medical specialists publications:
"Disorders of attention and consciousness.
. From amongst full qualitative
disorders of consciousness, depersonalisation appears, which of course is
not a specific symptom of schizophrenia.
As a special form of the above sometimes a narrower
concept is being singled out, so called apersonalization, when the
patient lives convinced that inside him resides also one alien personality, who
is forcing him to actions, which contradict his own conviction."
Rubner does not seem to appreciate that Dissociative disorders are a group, consisting of dissociative amnesia, dissociative fugue, dissociative identity disorder (D.I.D.), depersonalisation disorder, and dissociative disorders not otherwise specified. He calls the whole group of Dissociative disorders "Multiple personalities"[34] and considers them to be "hysterical neurosis."[35]
This is a simplistic view leading to the wrong diagnosis.[36]
Any attempt to explain dissociative disorders on the basis of the old concept of conversion neurosis [hysterics] is doomed to become a failure. Rubner identifies with the Hubers textbook definition of D.I.D.:[37] "Huber backdates the whole syndrome to the proximity of neurosis and hysterics, conversion neurosis and conversion hysterics and with this into the field of conversion neurotic disturbances." Contemporary psychiatry does not consider the group of dissociative disorders to be the hysterics of yesteryears.
From such a point of view of course the arguments Rubner is using loose their impact. The Dissociative Identity Disorder affected Karl May only during the years 18621874. Rubner thinks May suffered from hysterics his whole life. Neurotic or hysteric people do not experience true hallucinations; therefore Rubner assumed Karl May could not hallucinate either.[38] In 1891 the Swiss psychiatrist Anton Delbrück described what he named Pseudologia phantastica, a complex form of confabulation. This term has been ever since unjustly applied to Karl May, who was a creative writer.
Popular fiction represented a highly cultural function before 1950s. Popular fiction served as an escapist means of entertainment for the common people. However after the cultural equalizing post WW2, popular fiction came to be appreciated and studied with as much importance as high culture at an academic level. Recent post-modern cultural and literary analysis has shown how popular fiction and popular culture actually tends to reflect the psychological anxieties and pleasures of culture at large. Even if writers have oddities and expressions of individuality, to classify them as mentally abnormal is doing disservice to them.
![]()
![]()
![]()
References
Please click on the hyperlinked
reference numbers to return to your place in the text.
[1] Jürgen Seul: Karl May und die Justiz. Jb-KMG 2002. Husum 2002, pp. 275-315.
[2] Otto Rubner: 'Der sächsische Phantast. Eine Pathographie Karl Mays.' Jb-KMG 2003, pp.17-66.
[3] In (1), p.280: dass May nunmehr offenkundig bewusst und willentlich agierte, wofür die sorgfältige Planung und das kaltblütige auftrete, sprechen.
[4] In (1), p.283: Er [i.e. Karl May] bestätigte seine hochstaplerische Rollen, war sich ihrer also stets bewusst gewesen.
[5] In (4): Als multiple Persönlichkeit hätte ihm nie und nimmer die Einsicht kommen.
[6] In (4): In einem Dämmerzustand wird May seine Straftaten nicht begangen haben
[7] Thomas, W. E.: Karl May und die Dissoziative Identitätsstörung. Jb-KMG 2000, pp.195-231.
[8] American Psychiatric Association: Diagnostic Criteria from DSM-IV Washington, DC; Sixth printing, April 1999, p.230.
[9] In Germany the ICD-10-CM [International Classification of Diseases, 10th Clinical Modification] is also in use. There the former nomenclature Multiple Personalities is still noted, applying however only to D.I.D. and not to the whole group of Dissociative Disorders.
[10] Reference to "feeling like one is in a dream" from DSM-IV [in (8) p. 231], applies only to one of the Dissociative Disorders, to Depersonalization Disorder, an example of which is described later in (36).
[11] In (1), p.283: "dass in der modernen forensischen Psychiatric die Diagnose einer multiplen Persönlichkeiten als ein iatrogenes Artefact betrachtet (wird)."
[12] May, K.: Mein Leben und Streben. Olms Presse Hildesheim-New York 1997, p.111.
[13] See in (4).
[14] The Merck Manual Second Home Edition [Merck Research Laboratories, Division of Merck & Co., Inc. Whitehouse Station, N.J., USA, 2003] Section 7: Dissociative Identity Disorder - Contributor Richard P. Kluft, MD.
[15] Put forward by Mr. Ralf Harder.
[16] May, K.: Der Scout. In: Deutsche Hausschatz XV Jg. (18881889); Reprint: KMG Hausschatz 1997.
[17] Griesinger, W.: Pathologie und Therapie der psychiatrischen Krankheiten. Braunschweig 1871.
[18] See under (7).
[19] Kathrin Dornbusch, Abteilung Klinische Diagnostik/Intervention und Klinische Psychologie Friedrich Schiller Universität Jena, Am Steiger 3, Haus 1, 07743 Jena, Germany.
[20] "Die ganze Persönlichkeit des Angeklagten machte in der Hauptverhandlung den Eindruck eines komischen Menschen, der gewissermaßen aus Übermuth an der Anklagebank zu sitzen schien."
[21] In (17).
[22] Karl May: Mein Leben und Streben. Freiburg [1910], Reprint: Hildesheim-New York 1997, pp. 126-127.
[23] "Mit Verbüßung der Zuchthausstrafe verließ May auch seine kriminelle Laufbahn ". In (1), p. 285.
[24] Mitteilungen der Karl-May-Gesellschaft No. III., March 1997, p.49. Karl Mays words sound even more credible in the 21st century.
[25] THE AGE (Melbourne, Australia) December 26, 2002.
[26] See (2).
[27] Otto Rubners diagnosis of Karl May in: Otto Rubner: Der sächsische Phantast. Eine pathografie Karl Mays.: Im Rahmen der Konversionsneurose entwickelte er [i.e. Karl May] eine sehr erhebliche Fantasie, die in der Jugendzeit zu seinen einfallsreichen Delikten und spätter zu seiner schriftstellerischen Produktivität und zu der auβerordentlich wirksamen Anschaulichkeit der von ihm beschriebenen Figuren und Handlungen fűhrte. [In the framework of conversion neurosis he (i.e. Karl May) developed very considerable phantasies, which led in the youth to his resourceful crimes and later to his literary productivity and to the extraordinarily effective illustrative vividness of the by him described characters and action.], p. 59.
[28] According to (14) D.I.D. appears to be rather common; it can be found at present in 3 to 4% of people hospitalized for other mental health disorders.
[29] Diagnostic Criteria from DSM-IV. American Psychiatric Association, Washington, DC, 1999, pp.229-232.
[30] In (2): Ich selbst habe in meiner etwa vierzigjährige Tätigkeit als Psychiater . Die aufgefűhrten Symptomenkombinationen oder Krankheit niemals gesehen. [I myself have never seen in my about forty years of psychiatric practice the presented combination of symptoms or the disease.], pp. 57-58.
[31] Gast, U; Rodenwald, F; Nickel,V; Emmrich, H.M. (in press): Prevalence of Dissociative Disorders among psychiatric inpatients in German University Clinic. J. Nerv. Ment. Dis. Overkamp, B; Hoffman, A; Huber M. & Damann, G. (1997): Dissoziative Identitätsstörung eine Persönlichkeitsstörung? [D.I.D. A Personality Disorder?] Persönlichkeitsstörungen, 2, 74-84.
[32] U. Gast et alii: Diagnostik und Therapie Dissoziativer(Identitäts-) Stőrungen. Psychotherapeut, Heft: Band 46, Nummer 5, September 2001, pp. 289-300; Springer-Verlag Heidelberg.
[33] Mysliveček, Z., Prof., MUDr.: Speciální Psychiatrie. Prague 1956, pp. 158-159. The above quote is an English translation of the original Czech text [Stress by author].
[34] In Germany the ICD-10-CM [International Classification of Diseases, 10th Clinical Modification] is also in use. There the former nomenclature Multiple Personalities is still noted, applying however only to D.I.D. and not to the whole group of Disssociative Disorders.
[35] In (2): Die multiplen Persönlichkeitsstörungen würden fast nur in den USA diagnostiziert. Sie gehörten zu den hysterishen Persönlichkeitsstörungen, die der Pseudologia phantastica nahe ständen, und es handle sich um ein bewusstseinsnahes Syndrom oder sogar eine vorgetäuschte Tendenzreaktion. [The multiple personalities have been diagnosed almost entirely in the USA. They belong to the hysterical disorders of personalities, which stand close to Pseudologia phantastica and we are dealing with a consciousness close syndrome or even with pre-prepared deceiving intentional reaction.], p. 39.
[36] An example of Depersonalisation one from the dissociative disorders which in Rubners concept would be diagnosed as hysterical neurosis; from a narrative of WW2 concentration camp inmate: Susanna held fiercely to her loving memory of her brilliant father, Istvan, and learnt to stand [at dawn roll-calls on frozen ground] removed from her suffering as she willed herself to survive. Sometimes, you feel that maybe you were two people. One was the observer, and the other the victim. The Age [newspaper], Melbourne, Australia, 11 February 1999, p.13.
[37] In (2): Huber rückt das ganze Syndrom [i.e. D.I.D.] in die Nähe von Neurose und Hysterie, Konversionsneurose und Konversionshysterie und damit auf das Gebiet der konversionsneurotiches Störungen., p. 56.
[38] In (2): Die angeblichen Halluzinationen sind als Pseudo- oder Als-Ob-Halluzinationen und Ergebnis der lebhaften fantasievollen Verarbeitung des Zwangssyndroms anzusehen. [The alleged hallucinations are to be looked at as pseudo- or as-if-hallucinations and the consequence of a vivid reworking of the compulsive syndrome.], p. 55.
![]()
