Objective: To study the morbidity pattern of the elderly and to assess the treatment modalities.A Community Based Study of the Morbidity Profile among the Elderly in Chandigarh, India HM Swami, MD*
Vikas Bhatia, MBBS**
Rekha Dutt,MBBS***
SPS Bhatia****
Study Design: Community based, House to House, Cross sectional, Sample size selected by stratified random technique. Urban areas of Chandigarh.
Subjects: Three hundred and sixty two persons aged 65 years and above, 313 from urban and 49 from rural area.
Results: Among 362 elderly registered in the study, 153 were males and 209 were females. A large number of the subjects (89%) were suffering from at least one medical problem. Morbidity among rural subjects was observed to be less when compared to urban subjects. Females had higher rate of morbidity. Common presenting symptoms were pain/ swelling of joints (36.5%), limitation of movements (20.2%), indigestion/ heartburn (17.7%), backache (17.4%) and excessive tiredness. Medical history and physical examination by the physician revealed that most common diseases in order of the magnitude were hypertension (58%), osteoarthritis (50.55%),cataract (18.51%), gastritis (17.67%), deafness (13.53%) and diabetes mellitus/ hyperglycemia (12.15%). Anaemia (estimated by Haemoglobin estimation below 12 gm%) was recorded in 68.2% of the subjects. Study also observed that elderly with ailments were taking treatment in 68% of the conditions.
Conclusion: The study has highlighted the high prevalence of morbidity among elderly. Thus, there is an urgent need to develop geriatric health care services in developing countries on the basis of existing morbidity profile.
Bahrain Med Bull 2002;24(1):13-16.
Improvements in health care facilities have brought
about longevity which is considered
to be one of greatest achievements of the 20th
century. The ratio of older persons has changed dramatically from
approximately one in fourteen in the fifties to about one in four at present1.
Projections indicate that by 2020 there will be more than 700 million people
aged 65 years and above in the world, two third of them in developing countries2.
Three out of four countries projected to have the largest number of people
in the year 2025 are located in Western pacific and South East Asia: China,
India and Indonesia3. From the morbidity point of view, at least
50% of the elderly in India have chronic diseases4. This poses a greater
responsibility on health services especially in developing countries like
India where there is a greater strain on available health infrastructure.
Only limited data is available on problems of elderly in India which is
essential to develop, plan and evaluate the programmes for the aged. Thus,
the present study was carried out in rural and urban areas of Chandigarh,
a city located in Northern part of India, to find out the morbidity profile
among elderly.
METHODS
Union Territory of Chandigarh is having a population
of over 0.8 million5. Chandigarh also known as beautiful city, is situated
at about 250 kms from the national capital of New Delhi and is well acclaimed
for its good architectural planning, excellent educational facilities
and a network of health institutions.
STUDY DESIGN
The study was conducted in urban and rural areas
of Chandigarh having about 90% population in urban and 10% in rural areas.
The city has 47 sectors and 26 villages. Each sector is a unit. Therefore,
the list of all sectors with approximate number of households was prepared
and subsequently households were selected by stratified random technique
in proportion to the population in urban and rural area. The team visited
the selected number of the houses and enquired for the presence of any
elderly of the age of 65 years or more. Four villages were selected randomly
from the list of all villages. The number of households was decided on
the basis of population of the village. A total of 250 households in urban
area and 50 households in rural area were selected.
A team comprising of consultants, medical officer,
medical social workers, laboratory technician were given training in the
Department of Community Medicine, Government Medical College, Chandigarh,
so as to collect uniform information from the subjects. The team from the
department visited the selected number of houses and collected information
on a pre-designed and pre-tested format. The part-1 of format comprising
of general demographic structure of the family was collected by medical
social workers by interviewing with the subjects using interview technique.
Part II of the format, comprised of medical history
and symptoms. The male and female doctors using the interview technique
as per requirement collected data regarding the functional status of elderly.
A general and systemic examination was performed. Screening for hearing
impairment was assessed by using tuning fork and hearing test and vision
was tested by Snellens chart. The investigations were conducted at the
same time or appointment was given on following days as per the convenience
of the subjects. Investigations done in the study included haemoglobin
estimation by Sahlis method, random blood sugar by glucostics quick test,
ECG was done in all the subjects in their households by battery operated
machine. The data was entered in the computer and analysed on the FoxPro
programme. The study was done over a period of one year in 1998-1999.
RESULTS
In the present study, 1882 families having 7937 members were visited. There were 434 elderly in the study population and the proportionate geriatric population (65 years and above) constituted 5.47% of the total study population. Seventy-two were not included due to their non-availability in the families. Out of 362 subjects interviewed, 313 were from urban area and 49 from rural area, 153 (42.3%) males, and 209 (57.7%) females. Majority (66.6%) were in the age group of 65-74 years followed by 26.8% and 6.6% in 75-84 years and 85 years and above age group, respectively.
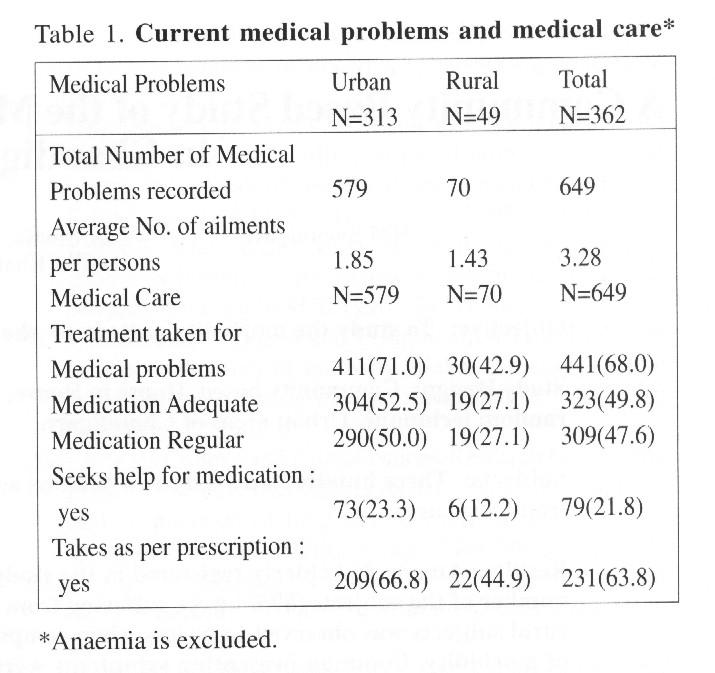
Total number of illnesses among 362 subjects was 649 as shown in Table 1. Anaemia was excluded from these medical problems. Therefore, average number of illnesses per persons was recorded as 3.28. At the time of survey, 88.9% of the study population was suffering from at least one ailment while 69.9%, 47.3% and 16.9% of population was suffering two, three and four or more ailments respectively. Table no.1 shows that only 68% of elderly were taking medicines for their illness and among them 73.24% were taking adequately, and 70.0% were taking on regular basis. Consumption of medicines was taken more adequately and regularly by urban subjects.
Morbidity among urban subjects was higher (90.7%)
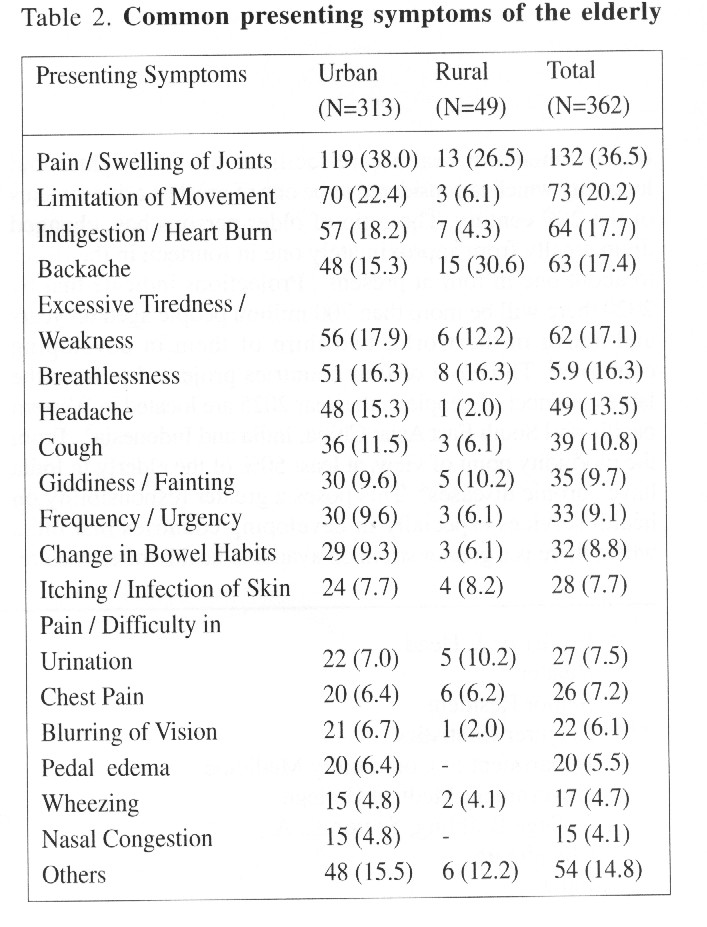
than rural (77.6%). Table 2 reveals the five common presenting symptoms
of the elderly were: pain / swelling of joints (36.5%), limitation of movements
(20.2%), indigestion/heartburn (17.7%), backache (17.4%), excessive tiredness/weakness
(17.1%). Most common diseases in order of their magnitude were hypertension
(58%) joint pains/arthritis (50.5%) cataract (19.1%), gastritis (17.7),
deafness (13.5%) followed by diabetes mellitus (12.2%), as shown in Table
3. Hypertension, gastritis, diabetes mellitus and arthritis were more common
illnesses in urban area whereas anemia (67.76%) and cataract (20%) were
more common in rural population.

Except for gastritis, the prevalence of common problems like hypertension, arthritis, cataract, deafness and diabetes mellitus was higher in females (Table 4). Prevalence of hypertension and diabetes was more in age group of 65-74 years. In rest of the commonly observed illnesses, prevalence increased with the age.

It was also observed in the study that 13.3%
of elderly were hospitalized during last one year which was more in urban
subjects. Thirty percent of subjects had undergone at least one surgery
in their lifetime and only fifteen percent of elderly had received tetanus
toxoid immunisation in the past five years.

Table 5 reveals that 31.8% of the subjects had
normal Haemoglobin (of over 12 gm%) whereas in the remaining 68.2% anaemia
was prevalent in different severity. Random blood sugar above 180 mgm%
was observed in 20.8% of the elderly. Similarly, different abnormalities
were noticed in ECG recording among 32.4% of the elderly.
DISCUSSION
The present community based study in the Union
Territory of Chandigarh with over 0.8 million population5 recorded a high
prevalence of morbidity (88.9%) besides two-third of the study population
was having anaemia. A study carried out in Southern part of
India reported similar results that is a prevalence of 82.9% in the
age group of 60 years and above6. The present study included the geriatric
population of 65 years and above as considered by WHO3. It is important
to make a cut off at 65 years for making global comparisons. This geriatric
age group constituted 5.47% of total population in Chandigarh. WHO reported
a proportion of 5% in developing and 15 % in the developed world3.
It was observed that average number of illnesses
per person was 1.79 and it was higher in urban community, which may be
due to a higher prevalence of hypertension and myocardial infarction among
them. Other studies among elderly in North and South India reported it
as 2.627 and 2.42, respectively6. The presenting symptoms of the elderly
are significant because patients report to health care providers with these
ailments. Thus, health workers and general physicians should be aware
of the underlying diseases related to these symptoms. The presenting symptoms
of the same disease may vary in elderly in comparison to younger population.
Most common symptoms in order of their magnitude were pain/swelling of
joints, limitation of movements, indigestion/ heartburn and excessive tiredness.
Prevalence of presenting symptoms did not match with the morbidity profile
because many presenting symptoms are not necessarily system specific eg.
heart burn in elderly could be the symptom of GIT or CVS. Breathlessness
could be a presenting symptom of anaemia, hypertension or bronchial asthma.
Many of the diseases were detected on examination and investigations which
the patient did not present as specific symptom. Therefore, the purpose
of highlighting the problem presenting symptoms is to make the treating
physician understand that presenting symptoms and actual disease may not
be co-relating.
Anaemia was the commonest with over two third
population suffering from it. The present study considered the haemoglobin
level of 12 gm% and below as anaemia for both males and females8. Anaemia
in the elderly may be multifactorial in etiology as nutritional, physiological
and pathological problems. It was observed that anemia was more in elderly
females. The higher prevalence of anaemia among women in the reproductive
age group is related to multiple pregnancies, nutritional imbalance, menstruation
and other gynaecological problems. Therefore, the resulting anaemia in
the reproductive age group continued to exist in elderly women, in absence
of any corrective measures. Fifty eight percent of elderly were suffering
from hypertension in accordance with the WHO report3. The present study
considered a person to be hypertensive with level of blood pressure higher
than 140/90 mm of mercury as per the WHO criteria9. The presence of hypertension
among the elderly in urban areas was about twice that in rural areas. It
could be because of sedentary and modern life style and stress in urban
areas. Hypertension was more in females as compared to males. Similar results
were also reported by other authors6,10. Nearly one third of
the study population had abnormal ECG recordings. It has been estimated
that approximately one quarter of all deaths in developing countries and
almost half of all deaths in developed countries are attributable to cardiovascular
diseases3.
A high prevalence of arthritis / joint pain in
the current study especially among females was also reported in other studies6,7.
Thus reflecting the hard life faced by women who never retire from household
work unless totally disabled.
Nineteen percent of subjects were suffering from
immature and mature senile cataract. It was more common in females and
the prevalence increased with the rising age. These results were in accordance
to another study11. Cataract was found to be more common in rural population
which may be due to increased exposure to ultravoilet radiation during
long hours of work in open fields12. The prevalence of blindness
in India is 14.9 per thousand population12. Eighty percent of this
blindness is due to cataract alone11. National blindness control programme
has an important role in reducing the quantum of cataract in the community
by organising eye camps13. A number of elderly were suffering from
Gastritis because of poor nutrition, increased use of non-steroidal analgesics
and indigestion owing to decreased physical activity. It was found to be
more common in males, similar to the results of other study7. Presence
of suspected diabetes mellitus in the elderly further reflects the increasing
life-style diseases in the community. And it was again almost three times
in females of that of males. In the term of health status, difference between
the male and female are clearly explicit in those females who have higher
rate of morbidity. In the process of caring and nurturing of other members
of the family women in India, invariably tend to neglect or overlook their
own well being. Prevalence of high morbidity among elderly needs strengthening
of geriatric health care services in accordance with the common existing
problems in the community. Preventive, curative and rehabilitative programmes
for the elderly are required for the control and management of later part
of the life.
CONCLUSION
The study among elderly in Chandigarh, India has highlighted a high prevalence of morbidity and identified common existing medical problems like anaemia, arthritis, hypertension, deafness, gastritis and diabetes mellitus. As there is a rapid expansion in number of elderly population, there is an urgent need to develop geriatric health care services in the developing countries like India and provide training to health care providers to manage the commonly existing health problems in the country.
REFERENCES
1. Holt PR. Approach to gastrointestinal
problems in the elderly. In: Yamada T,
Alpers DH, Owyang C,
et al (eds). Textbook of Gastroentrology. 2nd ed. Philadelphia:
JB Lippincott
Company, 1995:968-8.
2. WHO. Life in the 21st century. A vision
for all. The World Health Report 1998:5.
3. WHO. Epidemiology and prevention of cardiovascular
diseases in elderly people.
Technical report
series 1995; 853, 5,2-3,21.
4. Kumar V. Aging in India. Indian J Med Res
1997;106:257-64.
5. Directorate of census operation. Census of
India. General population tables and
primary abstract. Part
II-A and II-B. Series 28:1991.
6. Niranjan GV, Vasundhra MK. A study of health
status of aged persons in slums of
urban field practice
area, Bangalore. Indian J Com Med 1996;21:1-4.
7. Padda AS, Mohan V, Singh J, et al.
Health profile of aged persons in urban and rural
field practice area
of medical college Amritsar. Indian J Com Med1998;23:72-76.
8. Agarwal A, Advani SH. Anaemia. In: Sharma
OP, ed. Geriatric care in India.
Geriatrics and gerantology.
A textbook. 1st ed. India: AN B Publishers Pvt. Ltd,
1999:421-6.
9. WHO. Hypertension control. Technical report
series 1996;862:3.
10. Chadha SL, Radhakrishna S, Ramachandran
K, et al. Epidemiological study of coronary heart diseases in rural population
in Gurgaon district (Haryana State). Indian J Com Med 1989;14:141-7.
11. Mohan M. Survey of blindness
in India 1986-89. Results at a glance: All India estimates. In: Jose R,
ed. Present status of the National programme for the control of blindness
(NPCB). Opthalmology section, Directorate General of Health Services, Ministry
of Health and Family Welfare, Government of India: New Delhi,
1992:80-100.
12. Angra SK, Murthy GVS, Gupta SK,
et al. Cataract related blindness in India and its social implication.
Indian J Med Res 1997;106:312-24.
13. Park K. Textbook of Preventive and
Social Medicine. 15th edn. M/s Banarasidas Bhanot, Jabalpur:India
1997:307.
---------------------------------------------------------------------------------------
* Professor
& Head
** Reader
*** Senior Resident
**** Lecturer (Statistics)
Department of Community Medicine
Government Medical College
College Building, Sector 32-A
Chandigarh
India
![]()
![]()

Copyright 2001, Bahrain Medical Bulletin