Objectives: To study the management of hearing impaired Saudi children. This investigation was a part of an epidemiological study of hearing.The Management of Hearing Impaired Saudi Children.
An Epidemiological SurveyKamal J Daghistani, FRCSEd.*
Tarek S Jamal, FRCSI*
Siraj M. Zakzouk, FRCS **
Methods: Nine thousand five hundred and forty Saudi children below 15 years of age were surveyed. Each child was examined for hearing and various measures used for management of hearing impairment are discussed.
Results: Among the 9540 Saudi children surveyed, 1241 (13%) had hearing impairment and 782 (8%) were at risk of hearing impairment. A total of 1560 children received different treatment for the management of their hearing problems. Most of them were treated with systemic administration of drugs (50.83%) followed by surgical treatment (35.57%) for those who did not respond to conservative treatment. Topical drug administration was given to 21.47% of the children and hearing aids were chosen for 5.83%. Education and training methods were used in 4.61%.
Conclusion: It was observed that hearing impaired children required more than one modality for the proper management, whereas only one modality was effectively used for children at risk. Preventive measures e.g. family counseling, attendance of antenatal care of pregnant women, immunization, encouraging hospital delivery and early and proper management of pre, peri and postnatal infections and disorders has been highlighted.
Bahrain Med Bull 2002;24(1):7-9.
Childhood hearing impairment significantly affects
the acquisition, development and the use of language¹. The greater
the degree of hearing loss, the more difficult it will be for the child
to readily acquire language through the auditory channel. The most vital
need in the management of the deaf child is early diagnosis, which unfortunately
does not happen. It could minimize the consequences and help to introduce
early intervention. A
child diagnosed before 6 month of age has a huge advantage over one in whom diagnosis is delayed until 18 months of age. Therefore every effort should be made to identify the child with hearing loss as early as possible. Equally important is the early management of the childhood hearing impairment in order to protect children form the adverse effect of hearing loss on their educational development. Deafness and hearing impairment are major causes of disability in developing countries². Unfortunately, these are generally neglected as compared to other disabilities. The reasons for this are multiple. Principally, this is because, as in more developed countries, deafness and hearing impairment produce unseen disability. There is lack of awareness of the possibilities for prevention and uncertainties about methods of treatment and rehabilitation ². This study was undertaken to monitor various modalities used for the management of hearing impaired children in Saudi Arabia.
METHODS
A survey of 9540 Saudi children (4189 males and 5351 females) below the age of 15 years was carried out during Sept 1997 to May 2000. The sample selection was randomly designed with representation of children covering all socio-economic and demographic groups from different provinces of Saudi Arabia. Each survey team comprised of an ENT specialist, nurse, social worker, audiologist and field supervisor. After obtaining permission from the family, a questionnaire modified from WHO/PDH was filled in. This included age, sex, parent relation, pregnancy, labour, birth weight, family history, exposure to risk factors, immunization and past medical history. This was followed by the clinical ENT examination of the child. The hearing was assessed using free sound speech testing and tuning fork tests and a portable screening/audiometer was used testing frequencies of 1, 2, 3 KHz. Tympanometry was done for all the children. Those who failed the test or in doubt were referred to the audiology department in the main hospital of the area, where complete assessment of hearing took place. Pure tone audiometry using an interacuastic AC30 diagnostic audiometer and tympanometry using Grason Steadler GS133 admittance meter were performed for confirmation of the hearing status of the children. The very young and/or with profound hearing loss were referred for Auditory Brain Stem Evoked Response (ABR). Children considered at risk of developing hearing impairment included (a) positive family history of hearing loss (b) exposed to infection i.e. rubella, cytomegalovirus, syphilis, herpes simplex and toxoplasmosis (c) low birth weight 1,500 grm or less (d) hyperbilinubinemia (e) bacterial meningitis (f) neonatal asphyxia.Serology for those with positive history of TORCH infection were done. Children with discharging ear were swabbed for culture and sensitivity. The data were analysed by x ( test using EP-INFO
RESULTS
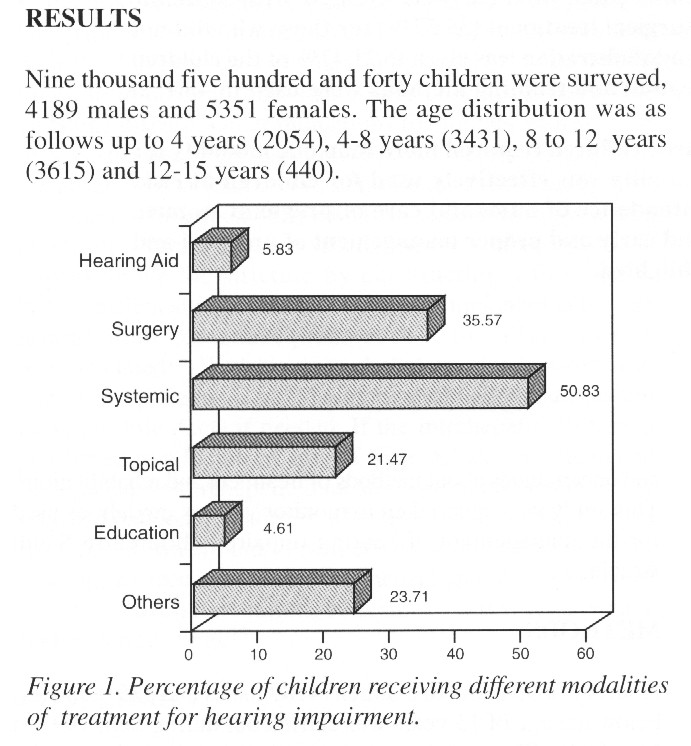
Nine thousand five hundred and forty children were surveyed, 4189 males and 5351 females. The age distribution was as follows up to 4 years (2054), 4-8 years (3431), 8 to 12 years (3615) and 12-15 years (440).
One thousand two hundred and forty one (13%) children had impaired hearing whereas 782 (8%) were at risk of hearing impairment. A total of 1560 children received different modalities of treatments for the management of hearing problems (Fig1). More than half (50.83%) of those treated received systemic antibiotics followed by surgical treatment in (35.57%) ie. myringotomy and insertion of ventilation tubes. Topical drug administration was given to 21.47% of children (topical antibiotics as gentamicin with corticosteriod, chloramphenicol and 1.5% acetic acid drops ) for those with discharging ears. Hearing aids were chosen for 5.83% of the children with impaired hearing. The use of education and training was effective in 4.61% of cases. Out of five hundred ninety nine children with Otitis media with effusion, 363 were treated by surgery (myringotomy with or without adeniodectomy or insertion of ventilating tubes). Anti-allergic medications (antihistamines, topical nasal corticosteroids and non-steroidal preparations) were used for those with a history of allergy.
Impacted wax was seen in 1229 (12.88%) which was removed. Chronic suppurative Otitis media was observed among 125 (1.3%) of children surveyed. Systemic and topical antibiotics were used and tympanoplasty was performed on 23 patients, the rest either refused surgery or were too young or did not report for follow up. Otitis media with conductive hearing loss was seen in 10.5% of the children surveyed, 1.5% with sensorineural hearing loss and 1.1% with mixed hearing loss.
Audiological assessment of the hearing impaired children showed that a total of 1.27% of the children had hearing impairment in the left ear and 2.26% in the right ear whereas 9.17% had hearing impairment in both ears. Moderate hearing impairment in left ear was seen in 22.7%, in the right ear 19.6%, compared to 13.4% in both ears. Hearing aids were prescribed to 334 children according to the degree and nature of hearing loss and motivation to use the aid. Hearing aids were fitted in one or both ears. Only 186 were able to purchase the aid.
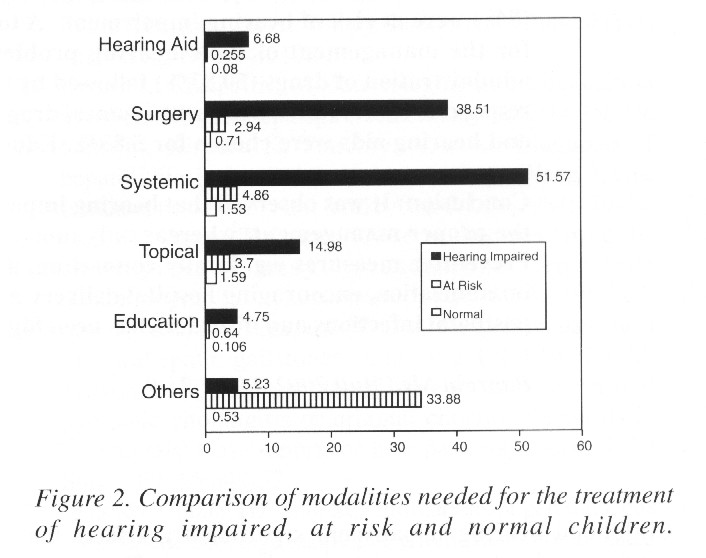
It was also observed that hearing impaired children
required more than one modality for the proper management of their hearing
problems, whereas only one modality was effectively used in at risk children
(Fig 2).
DISCUSSION
Children with hearing impairment are found
to have poor self perception than children of the same age with normal
hearing ³. Even relatively mild hearing losses may deprive the child
of approximately 50% of normal daily conversation with all subsequent complications¹.
The World Health Assembly in 1985, passed a resolution for the prevention
of deafness and hearing impairment. Much deafness and hearing impairment
are avoidable or remediable and developing countries had the greatest need
for the prevention and remediation of hearing problems². The
prevalence of childhood hearing impairment varies widely among different
populations. Naeem and Newton4 reported a three-fold higher prevalence
of sensorineural hearing loss (SNHL) in Asian children as compared to non-Asian
children. The prevalence of hearing impairment was reported to be
comparatively less (0.54 to 2.0 per 1000 children) in European children5-7.
Much higher prevalence of hearing impairment has been reported in Saudi
children8,9.
Our study showed that the prevalence of hearing
impairment was 13%. Our results also revealed that those with poor
antenatal care, failure to complete immunization, positive family history
of hearing loss and consanguinity had high prevalence rate of hearing impairment.
A total of 1560 children in our series received different modalities of
management for their hearing impairment. About half of them received
medical treatment followed by surgery in 35.7%. It was also observed
that hearing impaired children required more than one modality for the
proper management, whereas only one modality was effectively used in at
risk children. Surgical intervention for the treatment of complications
of ear diseases has increased in recent times. Tay and Mills10 reported
that 96% of the children suffering from otitis media with effusion benefited
from surgical treatment. Several investigators11,12 have reported
that surgery is a common practice for the management of cholesteatoma.
In our study 35.5% of the hearing impaired children were in need
of surgery. Tympanoplasty was performed in only 23 patients and 363
had myringotomy . Others refused surgery.
Only 186 were fitted with hearing aids. Patients have to purchase the hearing aid and since this is relatively expensive, not all who needed a hearing aid could afford it. It would be much more helpful if the aids were dispensed free. This was the practice of the health authority in Saudi Arabia till recently. It is left to people to purchase it on their own because of the high price and different sophisticated aids in the market. The issue of free hearing aid was restricted to those children enrolled in school for the deaf. The follow up information on the status of hearing in children fitted with hearing aids suggests the beneficial effects of hearing aids among that population13. Flanagan et al14 reviewed the acceptance and effectiveness of hearing aids in the management of children with persistent hearing loss due to Otitis media with effusion. They observed that 98% of the children had a definite improvement in their hearing, whilst using the aid. They suggested that the hearing aid is an effective treatment of deafness with high acceptance and compliance. In our study, almost all of the children who had myringotomy for O.M.E. improved and did not require hearing aid. De Maddalena et al15 have recommended the use of hearing aids for rehabilitation of hearing impaired population. Parental education plays an important role in early rehabilitation15,16.
CONCLUSIONS
This study showed a higher hearing impairment among Saudi children. Surgical treatment should be recommended for those who fail medical treatment. Hearing aids should be dispensed to those who need it whether they are in deaf school or not. Family counseling before marriage and immunization of girls and child bearing women against Rubella must be compulsory. Antenatal care attendance and delivery in hospital should be encouraged. Immunization should be compulsory for all children. Campaign of public awareness of hearing loss and its adverse affects on childs developmental through the media should be promoted.
REFERENCES
1. Ross M, Brackett D, Maxon AB. Assessment and
management of hearing impaired
children: Principles
and Practices. Austin, TX: Pro-Ed:1991.
2. Hinchcliffe R. WHO and its role in the prevention
of deafness and hearing
impairment [Editorial].
J Laryngol Otol 1997;111:699-701.
3. Maxon AB, Bracket D. The hearingimpaired
child: infancy through high school
years. Andover Medical
Publishers, USA:1992.
4. Naeem Z, Newton V. Prevalence of sensorineural
hearing loss in Asian children. Br J
Audiol 1996;30:332-9.
5. Davis A, Wood S, Healy R, et al. Risk
factors for hearing disorders: epidemiologic
evidence of change
over time in the LTK. J Am Acad Audiol 1995;6:365-70.
6. Darin N, Hanner P, Thiringer K. Changes in
prevalence, aetiology, age at detection
and associated disabilities
in pre-school children with hearing impairment born in
Goteborg. Dev Med Child
Neurol 1997;39:797-802.
7. Baille MF, Arnaud C, Caus C, et al. Prevalence,
aetiology and care of severe and
profound hearing
loss. Arch Dis Child 1996;75:129-32.
8. Zakzouk S, El Sayed Y, Bafaqeeh SA.
Consanguinity and hereditary hearing
impairment among
Saudi population. Ann Saudi Med 1993;13:447-50.
9. Bafaqeeh SA, Zakzouk S, ALMuhaimeid H, et
al. Relevant demographic factors and
hearing impairment in
Saudi Children; epidemiological study. J Laryngol Otol
1994;108:294-8.
10. Tay HL, Mills RP. The assessment of
hearing results following surgery for otitis
media with effusion
using the Glasgow Benefit plot. J Laryngol Otol 1994;108:733-5.
11. Schloss NM, Terraza O. Cholesteatoma
in children. J Otolaryngol 1991;20:43-45.
12. Wennmo C, Petersen H, Flisberg K. Cholesteatoma
surgery with the canal wall down
technique.
ORL J Otorhinolaryngol Relat Spec 1996;58:39-41.
13. Pitt T. Management and outcome: children
fitted with hearing aids in Ireland. Br J
Audiol 1995;29:199-207.
14. Flanagan PM, Knight LC, Thomas A, et
al. Hearing aids and glue ear. Clin
Otolaryngol 1996;214:297-300.
15. De Maddalena H, Reich K, Arold R. Significance
of parental variables on early
detection of paediatric
hearing loss. Results of retrospective survey of parents with
hearing-impaired
children. HNO 1997;45:30-35.
16. Meadow-Orlans KP, Mertens DM, Sass-Lehrere
MA, et al. Support services for
parents and their
children who are deaf or hard of hearing. A Natitional Survey. Am
Ann Deaf 1997;142:278-888.
------------------------------------------------------------------
*Associate Professors
King Abdulaziz University,
Jeddah
** Former Professor of Ear, Nose and Throat
King Saud University
Riyadh
Saudi Arabia.
![]()
![]()

Copyright 2001, Bahrain Medical Bulletin