Perianal Sepsis A Case Report
Alawi Hassan, MD*
Mohammed Abdul Saboor, MD**
Faiyza Haider, MD***
Mohammed Moheb, MD***
Perianal abscess and fistula are a cause of significant morbidity worldwide and have been documented since the time of Hippocrates ( 460 BC ). Anorectal sepsis accounts 0.5 - 1 % of all surgical admissions and constitutes 20- 25 % of those for colorectal disorders.
Except for unusual diseases, fistula in ano originates from infection in the anal crypts of Morgagni, forming an abscess which, when it opens, results in a tract leading to the skin surface. This brief report presents a case of fistula-in-ano with unusual aetiology that not reported in literature.
Bahrain Med Bull 2001;23(2):98-99.
Anorectal abscesses and fistulas are seen commonly in the primary care practice. An abscess forms as a result of obstruction of an anal gland, with resulting retrograde infection. Anal fistula simply represents the chronic phase of perianal abscess. The history is usually diagnostic and special studies usually are not required1.
THE CASE
A fifty year-old male presented to the local health center with history of sudden sever anal pain during defecation which was described as sharp as "insect bite". This was diagnosed as acute anal fissure and treated as such. Despite treatment the patient continued to have anal discharge which developed into throbbing pain which increased during sitting and coughing. Subsequenly, Perianal swelling developed followed by blood and pus discharge . A week later, he presented to the surgical clinic with main complaint of perianal swelling and blood discharge.
Patient gave no significant past history and his
systemic examination was normal. Local examination was suggestive of (perianal
abscess with fistula formation). He was scheduled for examination under
anaesthesia and anal fistulectomy.
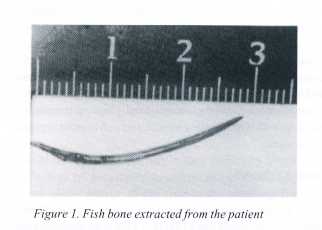
Peroperatively a foreign body (fish bone) was
seen inside the perianal abscess cavity (Fig 1), and a small opening connecting
to the anal canal could be identified. We treated the case as an anal fistula
and fistuolotomy performed.
Postoperatively, we asked the patient about history
of incidental fish bone ingestion. He was able to recall an incidence when
he propably ingested a fish bone and this was before his presentation.
Postoperative course was straight forward
and in subsequent visits to the clinic he had improved without complications.
DISCUSSION
Perianal abscess and fistula are fundamentally
the same condition, the abscess being the acute phase and the fistula is
the chronic phase. More than 90% of perianal abscesses are due to cryptoglandular
infection.
Associated diseases can predispose to anorectal
sepsis. Cronh`s disease (16 -20 % have anorectal complication), ulcerative
colitis (15% ), pulmonary TB, actinomycosis, lymphogranuloma venereum and
rectal cancer2. The incidence of fistula-in-ano following anorectal
abscesses was 26 % in the acute phase or as a sequelae3.
The symptom of perianal abscess is in the form
of a throbbing pain in the perianal region which is worse on sitting
and coughing4.
Fish bones are sharp objects and they can get lodged in the aerodigestive tract and cause complications, although this is rare-about 1% to 3% percent. but the associated complications are potentially catastrophic, including cervical abscess, mediastinitis, esophago-carotid fistula, lung abscess if it gets into the airway and perforated bowel as it passes through the intestinal tract.
The most common site for fish bone impaction is the esophagus and it comprises 60% of esophageal foreign bodies5. Plain x-ray films have 25 % sensitivity and 86 % specificity therefore, not a useful diagnostic investigation for fish bone impaction in the oesophagus6 .
In another study from Japan, plain films missed
about 56 % of fish bone impactions, whereas CT scan demonstrated the bones
in all cases7. PD Maldjian in 1999, reported two cases of small bowel perforation
secondary to ingested fish bones. In one of these, the findings from computed
tomography lead to the correct diagnosis preoperatively8.
In our case, a fish bone ingested by the patient
was impacted in the anal canal. The force exerted by the anal sphincter
during defecation or probably by the evacuated fecal matter resulted in
this sharp object being pushed through the anal wall with its pointed
end leading into the perianal tissue. Subsequently, infection resulted
in abscess and fistula formation.
A review of the literature revealed that
fish bones are not reported to perforate the large intestine or the
anal canal and not known to cause perianal sepsis. Therefore, it is unusual
for a sharp fish bone in the gastrointestinal tract to penetrate the anal
canal wall with its strong musculature and to cause perianal suppuration.
CONCLUSION
There are many causes of perianal sepsis, accidental fish bone ingestion is not one of them. This is an unusual case to be reported to highlight this rare cause.
REFRENCES
1. Hyman N. Anorectal abscess and fistula.
Prim Care 1999;26:69-80.
2. Chris M, Paul F. Anorectal sepsis, abscess
and fistula. J Surgery (Quarter edition)
1998;41: 69-72.
3. Henrichsen S, Christiansen J. Incidence
of fistula-in-ano complicating anorectal
sepsis: a prospective
study . Br J Surg 1968;7:371-2.
4. Lloyd-Jones W, Giles GR. The colon,
rectum and anal canal. In: Cuschieri A, ed. Essential Surgical
Practice.3rd edn. 1995:617.
5. Herranz-Gonzalez J, Martenz-Vidal J, Garcia-Sarandeses
A, et al. Esophageal
foreign body in adults.
Otolaryngol Head Neck Surg 1991;105: 649-53.
6. Ell SR. Radio-opacity of fish
bones. J Laryngol Otol 1989;103:1224-6.
7 Watanbe K, Kikuchi T, Katori Y, et al. The
usefulness of computed tomography in the diagnosis of impacted fish bones
in the oesophagus. J Laryngol Otol 1998;112:360-4.
8. Maldjian PD. Case Report : perforation
of the small bowel from fish bone
ingestion : CT
findings. J Emergency Radiology 1999;6:361-3.
---------------------------------------------------------------------------------------
* Consultant Surgeon
** Senior Resident
*** Resident
Department
of Surgery
Salmaniya
Medical Complex
State of
Bahrain
