Acupuncture helps people recover from drugs and alcohol problems. It
is used in clinics through the United States. Acupuncture can decrease cravings
for drugs and alcohol, reduce withdrawal symptoms, relieve tension, and help
people relax. Acupuncture treatments, taken enough times, clear the mind, build
energy, and give a sense of well being. According to Chinese tradition, placing
acupuncture needles in the ear affect specific organs such as the liver and
kidneys. Western science has confirmed that acupuncture treatments change levels
of chemicals in the body and act on the nervous system. Acupuncture itself is
not a substitute for therapy but is used in addition to counseling and self-help
programs.
How it all began
One day in the early 1970's, H.L. Wen, MD., then the only neurosurgeon in all
of South China and Hong Kong, was preparing to use electro-acupuncture as
surgical analgesia and the patient, who happened to be experiencing withdrawal
symptoms from opium at the time, reported his symptoms had disappeared. Wen
canceled the surgery and scouted the hospital for other patients in withdrawal.
He gave his pre-op procedure to them and their symptoms also ceased. Acupuncture
for substance abuse was born.
Why Acupuncture for Detox?
Reduces the physical symptoms of withdrawal
Relieves depression, anxiety, and insomnia.
Profoundly relieves withdrawal symptoms including cravings, body aches,
headache, nausea, sweating, muscle cramping, etc.
The acupuncture detoxification program is an ideal partner with other programs.
It alleviates withdrawal symptoms so mental and physical stability are quickly
achieved. This gives a new level of comfort allowing for more effective
counseling. Twelve Step program participation, or participation in any other
treatment program is considered important to sobriety.
In addition, acupuncture...
Can be used safely with any other health condition.
Does not utilize other abusable, addictive drugs for treatment
Can be effectively done on an outpatient basis.
Is successfully used as a drug detoxification method at over 100 different drug
treatment clinics in the United States and is also successfully used for this
purpose in at least 25 other countries.
Acupuncture Treatment
Five tiny needles are placed in each ear, and then the clients rest quietly for
45 minutes. This is a good time to relax, meditate or think about changes to be
made in your life. In detoxification treatment, points in the ear correspond to
specific organs including the lungs, liver, kidneys and nervous system. One of
the points is for relaxation. The treatment triggers the release of natural body
chemicals, including endorphins, which help reduce cravings for drugs, ease
withdrawal symptoms, and increase relaxation.
How Will I feel During the Treatment?
Once the needles have been placed, your ears may tingle or feel warm. Some
people even fall asleep. These are normal responses. Some people say they feel
very relaxed when they are having a treatment, other's don't feel much at all.
Even if you don't feel much you are getting benefit from treatment. Acupuncture
is most effective after a series of treatments over a period of time.
The Detoxification Process
During detoxification, your body filters out the toxins that you have been
storing up. Blood circulation begins to improve. Sometimes during the
detoxification period you may feel achy, not sleep well, be cranky, or even have
drug dreams. Please let the acupuncturist know if you have any of these symptoms
so that additional acupuncture points can be added to your treatment.
How to Receive Maximum Benefit From Treatment
Treatment time should be used to sit quietly, relax and reflect or meditate.
Do not smoke cigarettes or drink coffee in the half hour before and after
treatment.
Let the acupuncturist know if you have any health problems.
Get daily acupuncture treatments for the first two weeks, then
three treatments a week for several weeks, then two treatments per week for
several additional weeks. Final treatments should be once a week. If relapse
occurs or something stressful happens in your life, then additional treatments
are recommended.
Acupoint Locations
One of the most difficult tasks to perform at the California state board
examinations is the point location portion of the exam.
The problem is that the way in which students are taught to locate the points
are often different from the way in which the proctors locate the points at the
exam. When asked for details on how these points are actually located, the
acupuncture committee always says the same thing. Read CAM. CAM stands for the
title of the book; "Chinese Acupuncture and Moxibustion".
We've all read the way in which the points are located in this book, and there
are many point location descriptions that are very poorly stated. Very poorly
translated. We couldn't find these points if our livelihoods depended on it,
which they do.
I attended a workshop that was held by a former proctor for the state board
exam, Dr. Baljit Khalsa. He was very clear on how points are located in
accordance with CAM as decoded by the state board.
This article describes this decodification of how the AC proctors read the CAM
instructions for acupoint location.
Good luck Some key
points:
The proctors use their hands or use strings. Three proctors have to agree on the
location before they ink it with the invisible paint. They don't use cunometers,
or elastic bands. Doesn't mean you shouldn't, but since you wanted to
know...
Every point description in CAM says to see an illustration. If the illustration
is "figure" something. Then its a black and white illustration, usually found on
the same page, or nearby the page you're currently reading. If the instructions
on the point suggest that you see "col. fig.", that's a reference to a color
photograph, which are found at the end of the point location chapter, among the
extra points.
The position in which the limb is held when locating the points can alter the
location of the points rather dramatically. When we study point location in our
schools, we're often taught to hold the arm with the hand over the abdomen when
locating points on the large intestine channel, or with the hand over the chest
when locating points on the San Jiao channel. We must do away with what we were
taught in classes in favor of the position of the arm as illustrated in the CAM
book. This is the position that the limb will be when the points are found by
the state board exam proctors. Most of the arm positions, you'll find are with
the fingers pointing down.
Its all according to the book. However, there are times in which the text
description does not agree with the illustration. In this case, the text is
given priority. An example is for the point Stomach 34. The illustration shows
the leg straight, and the text suggests that the point is located with the leg
flexed.
You're damned if you do and you're damned if you don't. If you're a control
freak, now would be a good time to work on that. Let's move on...
Horizontal Cun on the upper
chest.
If you look to the nipple to determine your lateral four cun, think again. Or
rather, stop thinking that. Wiser to use the measurement from the supra-sternal
notch (Ren 22) to the acromium as your eight cun, or the supra-sternal notch to
Lung 2 for six cun. You can't rely on the nipple line for anything during this
test.
Horizontal Cun on the abdomen.
The rectus abdominis muscle is your four cun measurement lateral. On the lateral
boarder of this muscle is your spleen line. The midpoint of this muscle is your
2 cun measurement for the stomach channel.
First ICS versus the subclavicularfossa
>
If a point is in the subclavicular fossa, you find the space directly below the
clavicle. If a point is found in the first ICS you go to the sternal angle (aka
"Lump of Louie") and locate the first ICS based on the fact that the sternal
angle is the meeting point of the second rib. The ICS below the sternal angle is
the 2nd ICS. The ICS above it is the first.
>
Next to the midline, the first ICS is not the same as the subclavicular fossa.
The more lateral you go, the more likely it will be, but everybody is different.
On some people, there will be a difference between Stomach 13 and 14. On others,
there will not.
The Problem Points:
Lung 3 and Lung 4
Lung 3 and 4 don't show up on the test because the "radial" side of the biceps
is highly ambiguous. It changes depending on how you hold your hand. You can
look to the color figure that the text suggests, but you'll find that the black
words and lines for the channel are not lined up well, and so the channel that
should run down the lateral side of the biceps, travels down the middle instead,
where the pericardium channel should be found. This is a terrible illustration,
all because the black ink and the color photograph beneath were not lined up
well during the printing stage of this book.
Lung 7
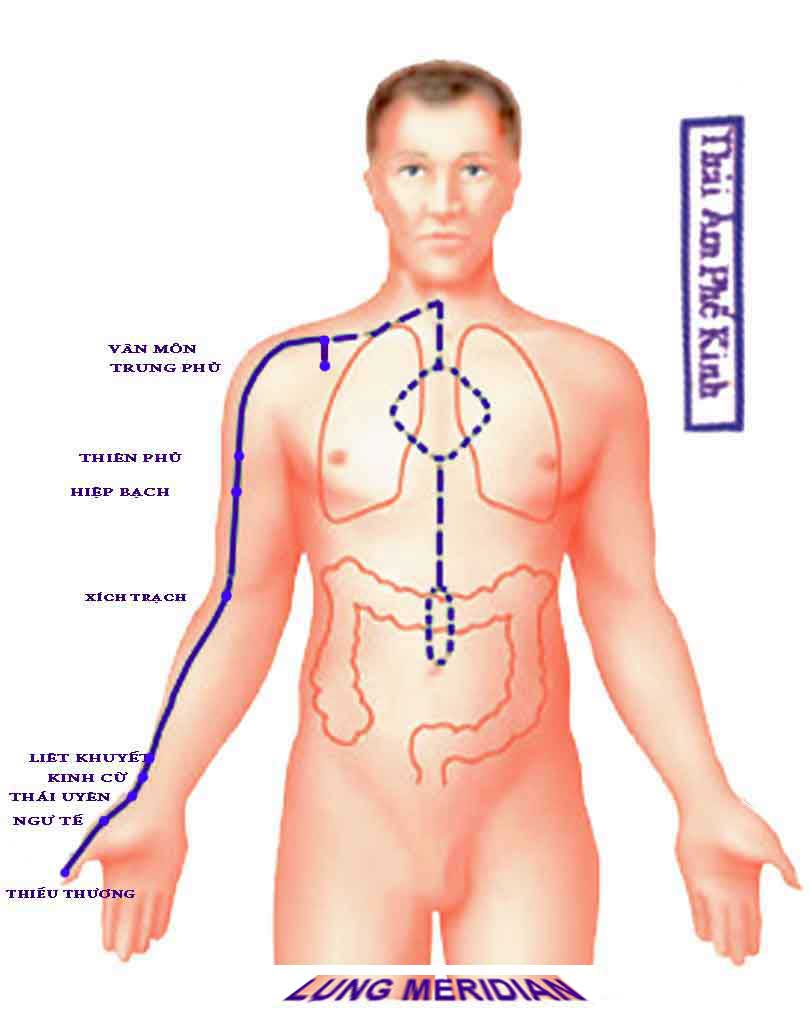
Lung 7 is located in the cleft superior (and adjacent to) the styloid process of
the radius, however, in the diagram, that location is shown to be on the Yin
side of the arm, closer to the course of the channel from Lung 5 to Lung 9. Keep
that in mind. Bring the point in toward the rest of the Lung channel just a bit
so its not so close to the LI channel. An half of an inch should do
it.
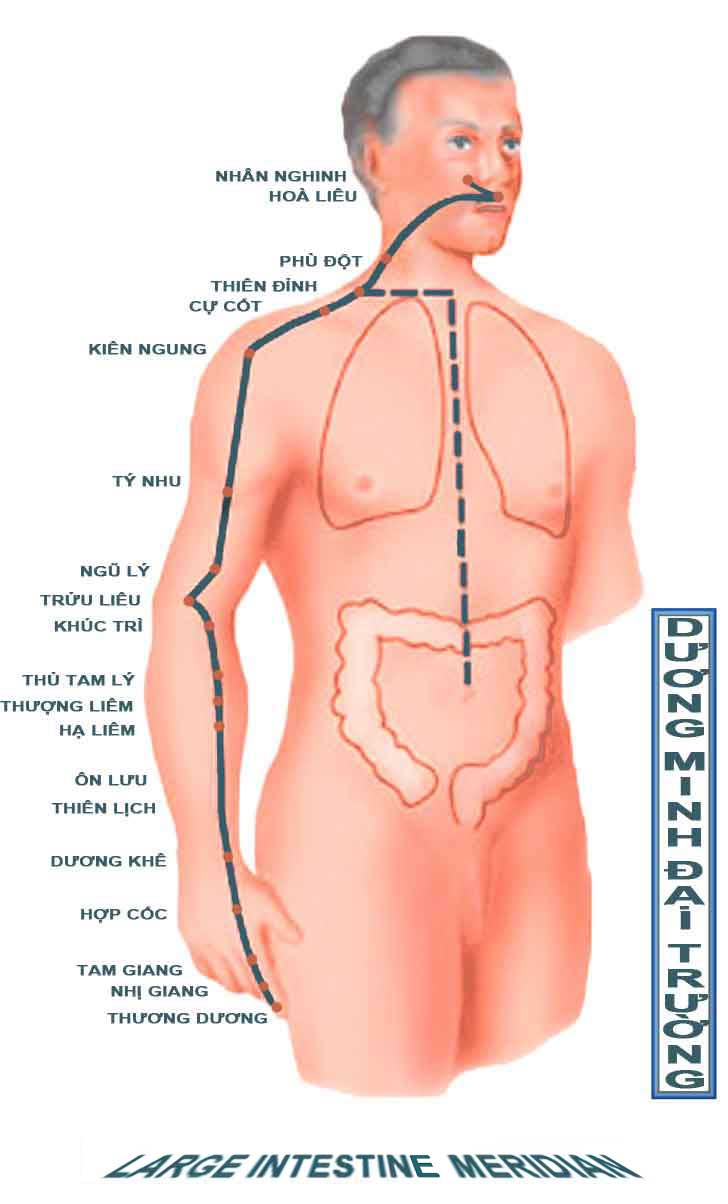 Large Intestine points on the arm
Large Intestine points on the arm
Notice that the elbow is slightly flexed in Figure 61. The point should be
located in the arm down position as in Figure 61.
LI 12
This point is a little funny. "Superior to the lateral epicondyle
of the humerous" is a tough statement. It should be noted that the epicondyle
makes a slope toward its widest part at the elbow. This point is at the
beginning of the slope, not at the wide part which is not superior to LI 11.
Ultimately, it would likely be more intelligent just to eyeball one cun superior
and lateral to LI 11.
LI 13
The 3 cun measurement is based on the Lung channel's nine from the axillary fold
to the elbow crease.
LI 14
The 7 cun measurement is based on the Lung channel's nine from the
axillary fold to the elbow crease. This point may or may not be at the very end
of the deltoid.
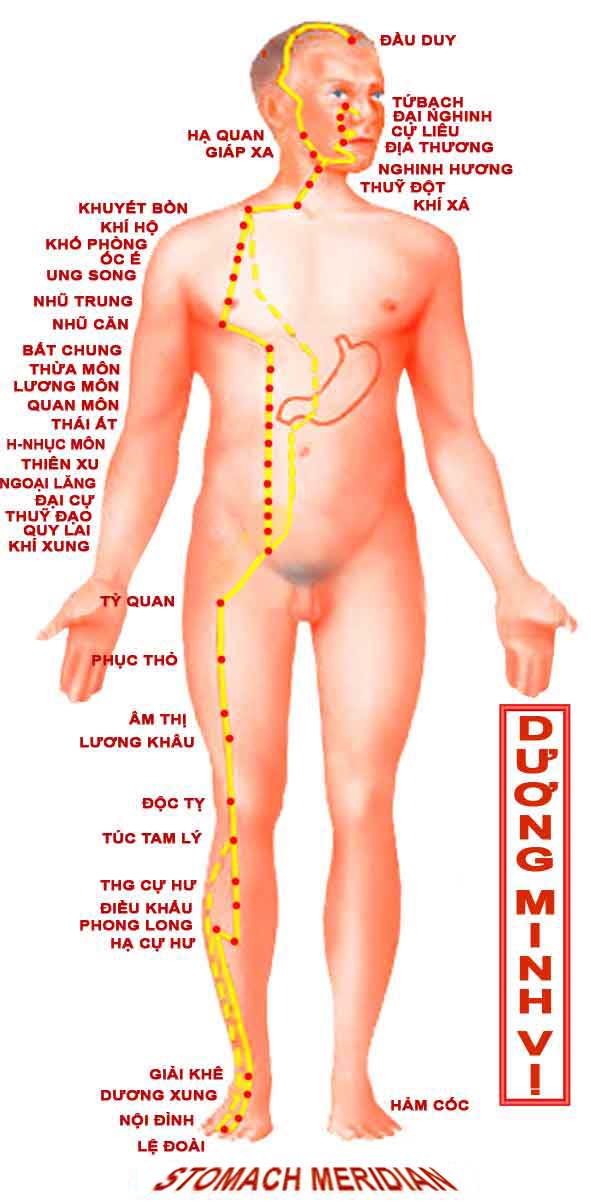
Stomach 32
Like Spleen 11, this is not an easy point to find on a standing
model at a test. If this point is used, it could easily be thrown out because of
the number of people who could potentially get it wrong.
Stomach 33
First, determine 19 cun (from the greater trochanter to the
patellar crease). Remove one cun from your measurement tool, such as a string.
Fold the string into half, and then fold it into thirds to obtain a valid three
cun measurement for the thigh. Now, use that three cun measurement to measure
from the laterosuperior border of the patella, upwards toward the ASIS as
suggested in CAM. And don't forget to glex the knee when you finally set the 3
cun measurement down on to the model.
Stomach 34
While standing, have the model stand on their tip toes to bring
out the tendon that connects to the top of the knee, as shown in figure 69 of
CAM. Place your finger there, lateral to the tendon, and have the model sit
down. Then, eyeball 2 cun up from the superior lateral corner of the patella,
using the model's hand if you chose, staying lateral to that tendon. That's
Stomach 34. Still a crap shoot, but its all I have to work with.
Spleen 10
Guestimate 2 cun based on the width of fingers or any other method
you chose. Then, with the knee flexed at 90 degrees, travel up the leg and
toward the midline (i.e. toward the groin) at a 45 degree angle from the
mediosuperior border of the patella.
Look for the highest point of the bulge of the muscle
located 2 cun above and medial to the patella. The highest point means the part
of the muscle that extends the furthest away from the femur. That's your point.
I don't think the placing of the palm on the knee is as good as eyeballing the
highest point of the bulge. The proctors are looking for that bulge. So should
you.
Spleen 11
>
This point was used recently in a test. It drew so much criticism
that it was thrown out. It shouldn't be used again. If it is, rejoice, because
you'll get that point, for sure.
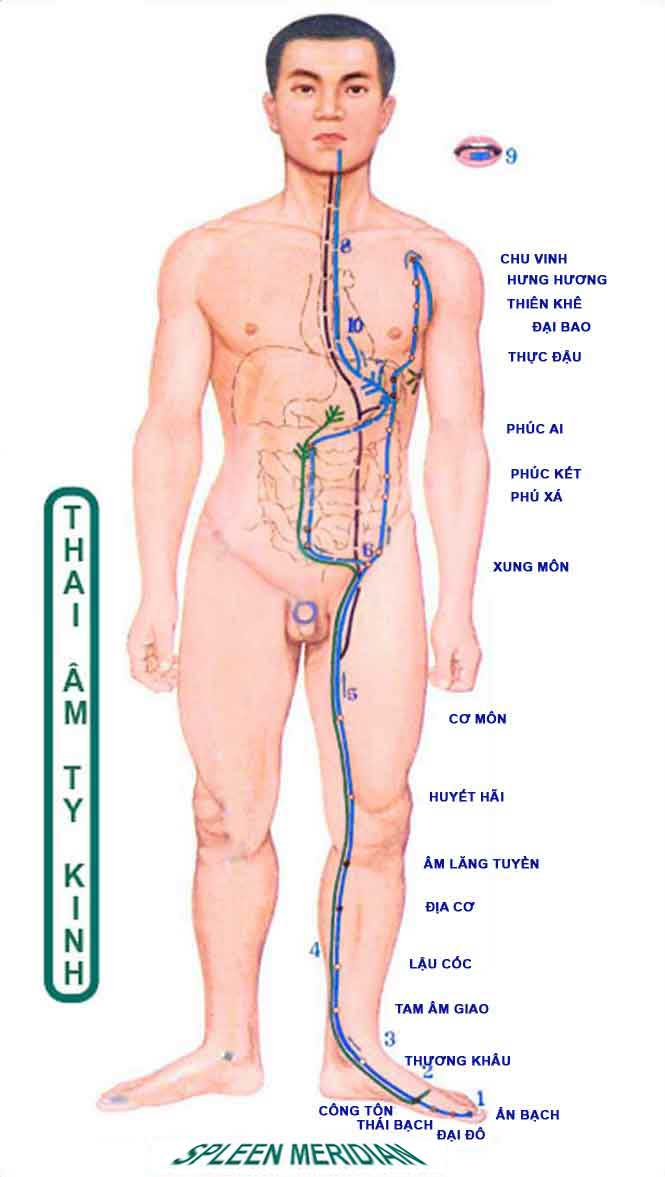
Spleen 14
/
How do you measure 1.3 cun? There is no official means.
Spleen 15
The lateral border of the muscle rectus abdominus determines your
measurement for the four cun lateral on the abdomen. Keep that in mind for your
Stomach and Kidney channel measurements too. The mamilary line is next to
impossible to determine with the model standing up, and it is an estimation at
best given the wide variety of chest sizes of both sexes.
Small Intestine 7
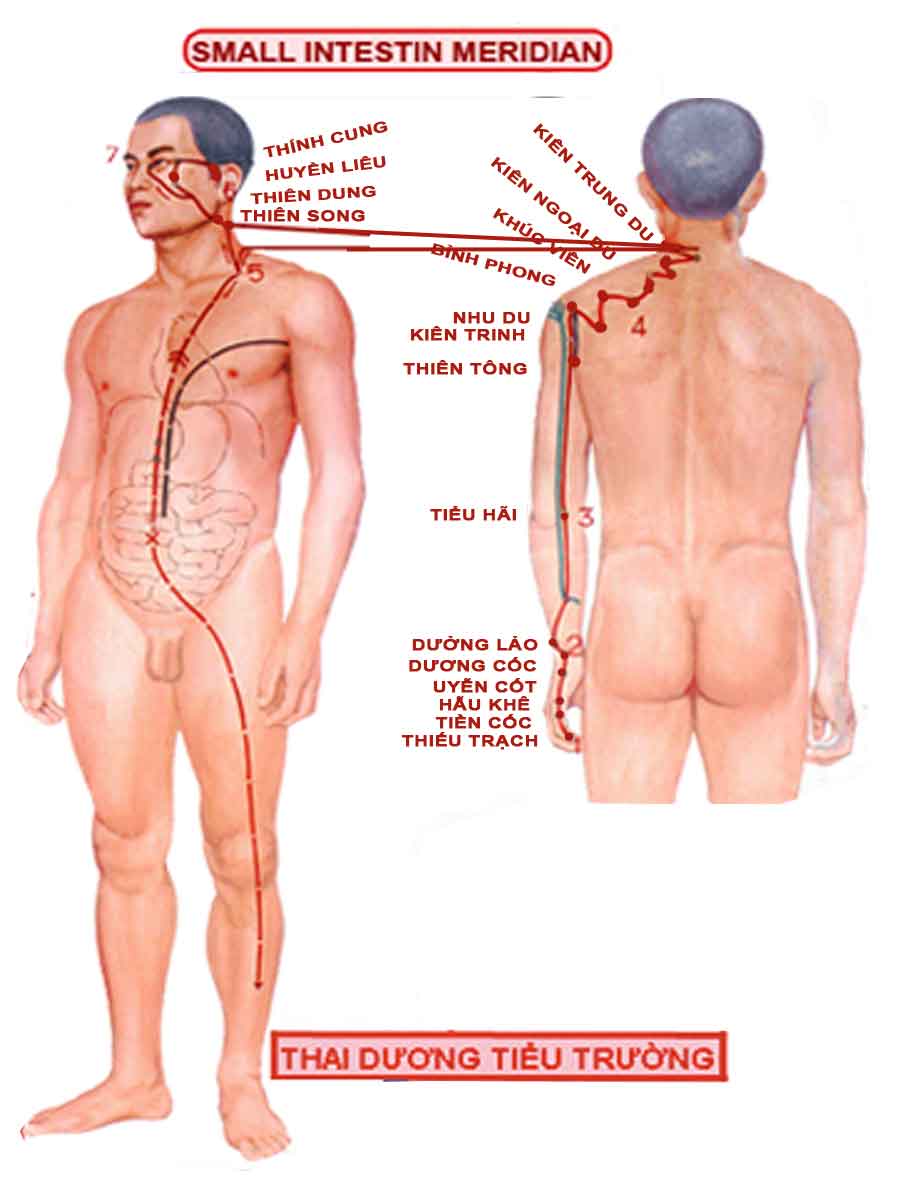
You'll see from figure 80 that the arm is pointing down.
That's the method by which the proctors will chose to locate the points. You
should too. The 12 cun for the Yang channels on the lower arm are based on 12
cun that extend from approximately Lung 5 to LI 5. Once you've got your twelve
cun, then pull that measurement over to the Yang side of the arm and put the
point on the line connecting SI 5 and SI 8.
Outer-Shu points:
Since the three cun measurement is based on the medial extremity
of the scapula, labels should be placed half on the scapula and half off (medial
to) the scapula. That way the label fully covers the correct point, nothing
else.
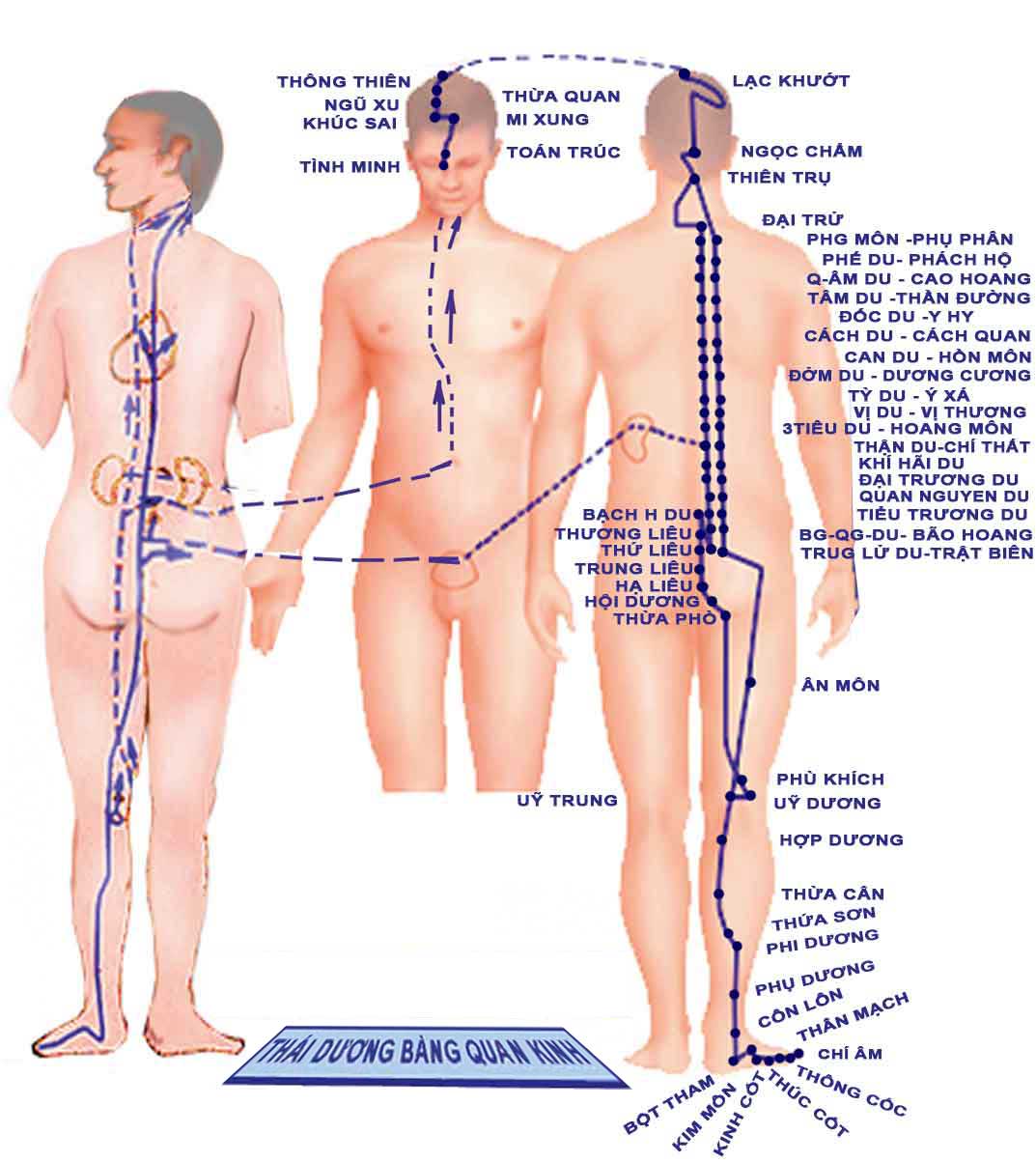
UB 56
Because UB 57 is based on a structure (the gastrocnemius muscle),
the instructions for this point cannot suggest a specific cun measurement below
UB 40. You find UB 55, which is 2 cun below UB 40, and then you find UB 57 which
may or may not be 8 cun below the transverse crease of the popliteal fossa. It
is below the gastrocnemius muscle.
UB 57
The book says that it is found below the belly of the
gastrocnemius, about 8 cun below UB 40. Well, which is it? Below the gastroc, or
8 cun below. The answer is that the proctors first find the gastroc, if it is
not about 8 cun below, then they'll find the 8 cun mark and place the dot in
between the gastroc location and the 8 cun location. Better to shoot for the
gastroc, rather than 8 cun mark.
UB 60
7 cun above UB 60 is more important than 1 cun inferior and
lateral to UB 57, though both should be taken into account.
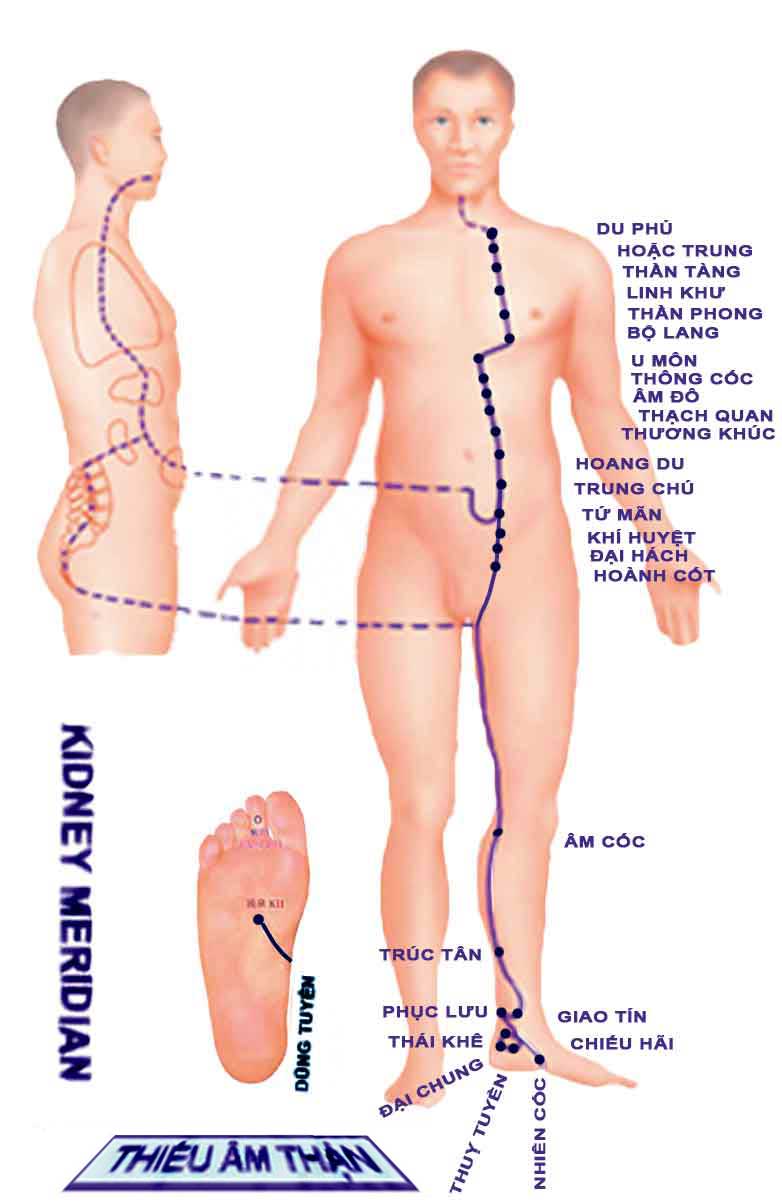
Kidney 9
The five cun here is based on the thirteen from Spleen 9 to the medial
malleolus.
Kidney 10
Find the point with the knee flexed to locate the tendons, then place the
sticker with the model standing up straight.
Kidney points below the umbilicus have happened before. Be aware of that.
PC 4
This point is initially located on the line that connects PC 3 and PC 7.
However, if it is not between the tendons, it should be relocated to fall
between the two tendons. That's what the proctor told us. I'm a little slow to
except this one. I think that the letter of the description in CAM is pretty
clear. The first sentence talks about the line from PC 3 to PC 7. Secondly it
talks about the tendons. Seems like the line is more important. Sorry that this
is ambiguous. After four years of TCM training, you should be used to it by
now.
San Jiao Points on Lower Arm
The arm is in the down position as shown Figure 96. Again the 12
is based on the length from the crease of the elbow and the wrist crease on the
Yin side of the arm where it is most easy to locate.
SJ 13
Draw a line from SJ 10 to SJ 14. SJ 13 is located at the point
where this line intersects the border of the deltoid. I personally think of this
as the inferior border of the deltoid muscle, but because the border is as much
vertical as it is horizontal, the makers of CAM called it the posterior border.
Same difference. The intersection of the border of the deltoid muscle with the
line drawn from SJ 10 to SJ 14.
GB 14
This point has shown up in past exams. It could again. The middle of the eyebrow
can change for a variety of reasons. You should orient the point directly above
the pupil of the eye.
GB 21
.
Follow the order of the instructions in the book. First, locate
the midpoint of the line that extends from Du 14 to the acromium. Then roll up
to the highest point of the shoulder. This isn't really the portion of the
shoulder that is the highest, which would be closer to the neck, but this is the
top of the shoulder, the superior aspect, still directly above the midpoint of
the line described prior.
GB 22
.
The arm should extend away from the body 90 degrees (making it
horizontal) when finding the axila point to begin the 12 cun measurement that
extends to the tip of the 11th floating rib.
GB 31
.
Because the length of arms and hands vary widely, it is safer for everyone
involved to use the 7 cun measurement for this point.
Regarding what "lateral aspect of the thigh" means, please see "Fig 106". In
this diagram, you'll see that the point is immediately posterior to the shaft of
the femur. Although this can be a little difficult to palpate, we do have a clue
as to what "lateral aspect of the thigh" officially means. Posterior yet
immediately adjacent to the femur.
GB 33
This point is rarely found 3 cun above GB 34. It is a little further than that
on everyone in the workshop I attended. Rather, there are some reasonably
specific physical landmarks that should serve to limit any ambiguity regarding
this point.
This point is in the depression at the bottom, or inferior end of the groove
between the lateral condyle of the tibia and the tendon of the muscle biceps
femoris. These two landmarks create a depression that rises up the thigh. Within
this groove, five cun above the popliteal crease, is where you'll find GB
32.
You could say that GB 33 is the Liver 8 of the Gall Bladder channel.
Liver 5
The question with this point is whether the point is located on
the bone as some more esoteric practitioners teach, or posterior to the bone
which would enable a more perpendicular needle insertion. The answer is in
figure 110 of CAM. The point is located, officially posterior to the tibia.
However, since the point is posterior and adjacent, practically touching the
bone, it would be prudent to place your label half on the bone and half off the
bone so as to put the actual point right in the middle of the label.
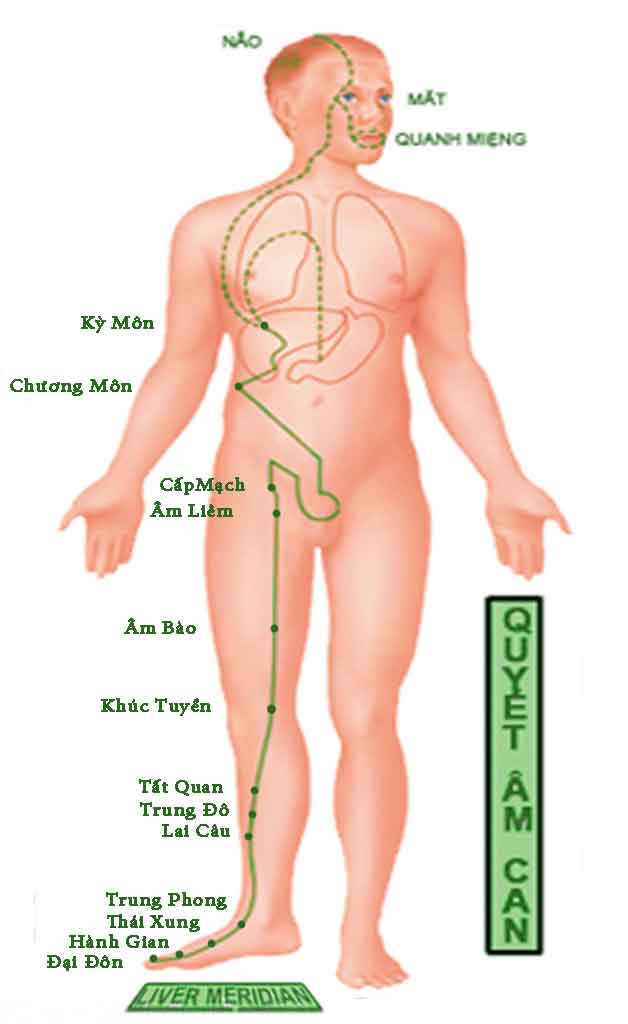
Liver 8
This point frequently shows up in state board exams. The point is
located with the knee bent as shown in figure 111. Notice that the knee is bent
about 90 degrees.
"under contruction"