|
|
|
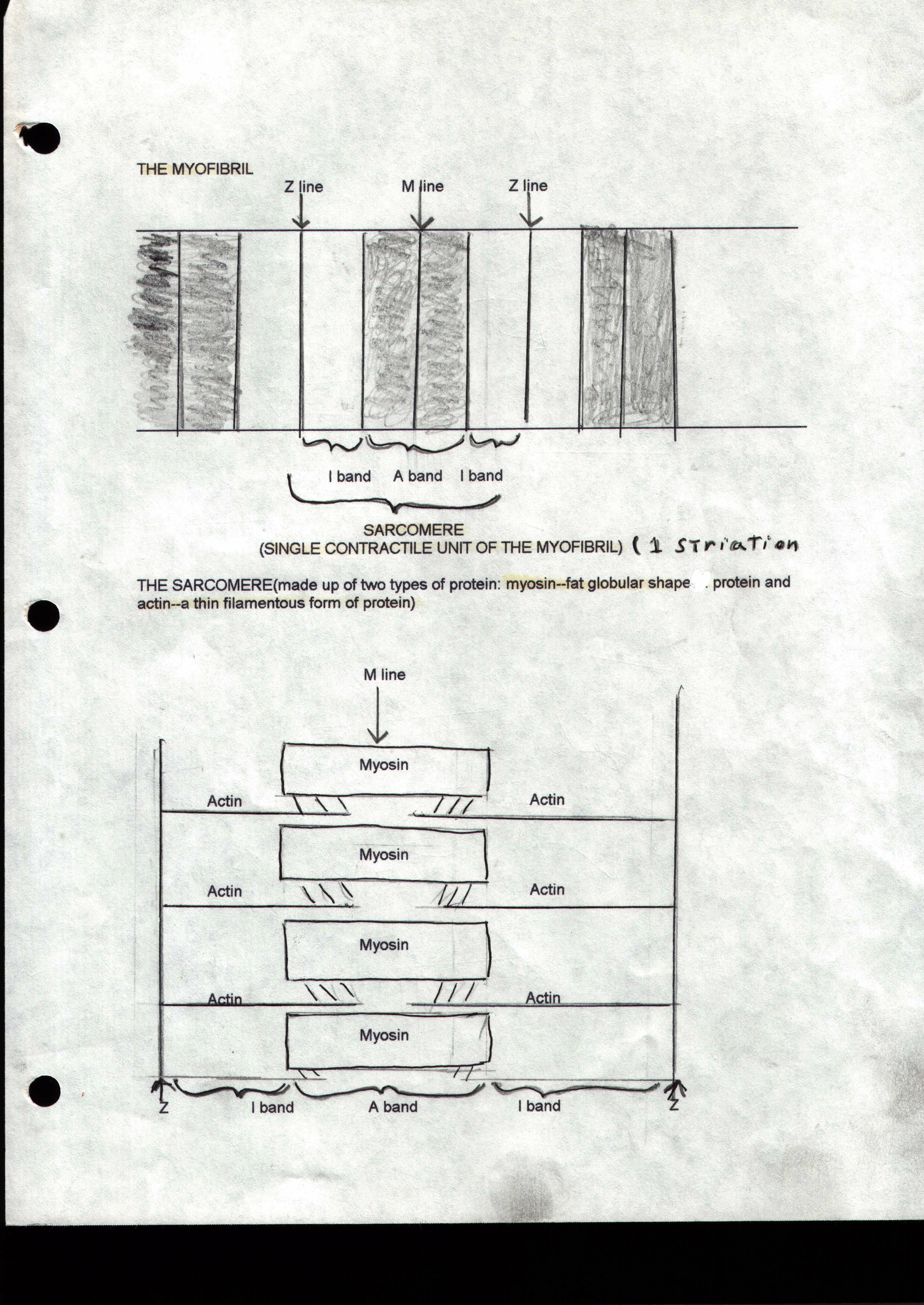
SKELETAL MUSCLE I) Structure of a Skeletal Muscle: Each muscle is surrounded by a dense irregular sheath of connective tissue called the epimysium. Each bundle of muscle fibers called a fascicle is covered by a layer of fibrous connective tissue called the perimysium. Each muscle fiber within the fascicle is covered by a layer of connective tissue consisting of mostly reticular fibers called the endomysium. All three connective tissue layers converge and join with each other to form the tendon so that when the muscle fibers contract they pull on the connective tissue sheaths which forms into the tendon transmitting the force along the tendon to move the bone. II) Skeletal muscle interaction: 1) Skeletal muscles are attached to bones by tendons. The two points at which they are attached are called the point of insertion (attachment on the bone that it moves) and the point of insertion (attachment point of attachment). As a muscle shortens or contracts it moves toward the point of insertion resulting in a "pulling" force on the bone that it moves. 2) Muscles are classified into four functional groups: a) Prime movers or agonists are muscles that produce a particular force that produces a specific movement such as the biceps brachii which inserts on the radius and flexes the elbow. b) Antagonists are muscles that oppose or reverse a particular movement and are located on the opposite side of the agonist. The antagonist of the biceps brachii would be the triceps brachii. The triceps will relax when the elbow is flexed by the biceps or it may be partially contracted to slow down or even stop flexion of the elbow. The triceps brachii when contracted will extend the elbow and then can be classified as the prime mover and then the biceps becomes the antagonist c) Synergists are muscles which help prime movers perform their movement by adding extra force or they can be used to reduce unnecessary movement as the prime mover contracts such as the synergists which stabilize our wrist as we make a fist. The tendons of the flexor muscles of our fingers cross both the wrist and the phalangeal joints. Synergistic muscles in the wrist stabilize the wrist as we make a fist or our wrist would bend as we make a fist. d) Fixatiors are muscles that immobilize a bone or a muscle's origin. Examples would include the muscles that contract and cause us to maintan an upright posture. III) Microscopic Anatomy of a Muscle Fiber: a)Each muscle fiber is a long cylindrical cell with multiple nuclei (syncytial) within its plasma membrane called the sarcolemma. Within the sarcolemma of the muscle fiber is the sarcoplasm or cytoplasm of a muscle cell or fiber. The sarcoplasm differs from the cytoplasm of other cells in that it contains large amounts of glycosomes (stored glycogen) along with an oxygen binding protein called myoglobin. The usual organelles are present and packed between sometimes a thousand rodlike structures called myofibrils which run the length of the muscle fiber. The myofibrils are the contractile elements of the skeletal muscle cells. b) Striated muscles are said to have striations or stripes. These striations are due to the presence of two types of protein found within the myofibrils. A globular protein known as myosin and a long filamentous protein called actin. Each myofibril is divided into individual contractile units called sarcomeres which contain layers of myosin and actin in such a way as to form the striped appearance of skeletal muscle that we see under the microscope. Each stripe or striation, if observed closely can be divided into different bands. A sarcomere is the region of a myofibril between what is known as the Z discs or Z lines. These are where a single sarcomere begins and ends. In the middle of each sarcomere is the stripe or striation that we see under the microscope. There is actually a series of repeating dark A bands (stripes in the middle of the sarcomere) and light I bands. The I bands have a midpoint dark line interruption called the Z disc that we just mentioned. The A bands also have a midpoint dark line interruption called the M line. The M line appears only in a contracting muscle and a lighter band appears in a resting muscle called the H zone. c) The Z lines are composed of proteins called connectens which act to connect each sarcomere with each other so that they can contract as if one unit within the myofibril. The I bands consists of thin filamentous protein molecules called actin which are inserted between larger myosin molecules within the A band. The I band therefore consists of actin molecules only and the A band consists of alternating layers of myosin and actin molecules and is why the A band appears much darker. When a muscle contracts the actin molecules slide between the myosin molecules in successive sarcomeres. The M line is composed of fine protein or desmin strands that hold adjacent myosin molecules together.
d) Myosin molecules have a rodlike tail consisting of two interwoven heavy polypeptide chains. At the ends of the heavy chains are two swollen areas called heads. They are swollen because of the attachment of a lighter polypeptide chain. The "head" are also called the cross bridges because they link the thick filaments of myosin with the thinner actin filaments during contraction. Each thick filament contains about 200 myosin molecules and are bundled together in such a way that their tails form the central part of the filament and their heads facing outward and in opposite direction. The heads of the myosin molecules contain ATP binding sites and ATPase enzymes that generate energy for muscle contraction. e) Actin molecules are polymers which are large molecules made up of many smaller molecules bonded together called monomers. The monomer for an actin molecle is called globular actin or G actin. The G actin molecules bear the active sites to which the myosin molecules attach. Each actin filament bends back on itself and winds around itself forming a helical structure. Two strands of tropomyosin which is a rod shaped protein spiral around the actin core. Tropomyosin is a regulatory protein and in a relaxed muscle state bock actin's active site so that the myosin heads cannot bind to the thin filaments. Another regulatory protein is a thin filament called troponin which forms a three-polypeptide complex or a troponin complex. One of the three polypeptides (TnI) is an inhibitory subunit that binds to actin. Another (TnT) binds to tropomyosin and helps to position it on actin, while a third one (TnC) binds calcium ions. IV) The Sarcoplasmic Reticulum (SR) acts to regulate intracellular levels of ionic calcium in that it stores calcium and releases it on demand when the muscle fiber is stimulated to contract. The SR is the endoplasmic reticulum of the muscle cell and consists of interconnecting tubules that surround each of the myofibrils. The tubules run longitudinally along the myofibrils and some form perpendicular cross channels called terminal cisternae (end sacs) at the A-I junctions and they also occur in pairs. V) The T tubules or transverse tubules are elongated tubes formed at the A band-I band junction by the sarcolemma penetrating into the cell at this point. The lumen (inside of each T tubule) is continuous with the extracellular space. Each T tubule runs between the paired terminal cisternae of the SR forming triads (successive groupings of the three membranous structures of a Tubule between two terminal cisternae). The T tubules also encircle each sarcomere as they pass from one myofibril to the next. The T tubules can conduct impulses from the sarcolemma to each of the sarcomeres. These impulses signal for the release of calcium from the adjacent terminal cisternae. IV) Contraction of a Muscle Fiber I) The Sliding Filament Mechanism of Contraction
2) The Neuromuscular Junction and the Nerve Stimulus a) An impulse or a message sent from the brain through a nerve cell called a neuron. The point at which the end of the neuron (the axon) reaches the muscle is called the neruomuscular junction. The axonal endings and the muscle fiber are very close and remain separated by a space called the synaptic cleft. The synaptic cleft is filled with a gel-like extracellular substance rich in glycoproteins. Within the axonal ending are synaptic vesicles containing a neurotransmitter called acetylcholine (ACh). The muscle fiber's contribution to the neuromuscular junction is the motor end plate and is highly folded providing a large surface area for the millions of ACh receptors found there. b) When the nerve impulse reaches the end of an axon calcium channels in its membrane open, allowing calcium to flow in from the extracellular fluid. The presence of Calcium inside of the axon terminal causes some of the synaptic vesicles to fuse with the axonal membrane and release ACh into the synaptic cleft by exocytosis. ACh diffuses across the cleft and attaches to the ACh receptors on the sarcolemma. At this point electrical events are triggered here that take place in excited nerve cell membranes (figure 9.9) 3) The Muscle Twitch and the Development of Muscle Tension a) The response of a muscle to a single brief threshold stimulus is called a muscle twitch, during which the muscle contracts quickly and then relaxes. The muscle is attached to an apparatus called a myogram which records the contractile activity graphically. Three phases are apparent in a myogram: 1) Latent Period: the first few milliseconds after muscle stimulation during which excitation contraction coupling is occurring (figure 9.10). Muscle tension here is beginning, but no response is seen on the myogram during this period. 2) Period of Contraction is when the cross bridges are active from the beginning to the end of tension development. The myogram peaks and this period lasts for 10-100ms. 3) Period of Relaxation is the final phase lasting 10-100 ms and is initiated by reentry of Calcium into the SR. Contractile force decreases to zero and the tracing returns to baseline. The muscle now returns to its normal length. **twitch contractions can be rapid and brief as with eye movements or can occur more slowly during which the muscles can remain contracted for longer periods such as in larger muscles like the gastrocnemius and the soleus (figure 9.12).
b) Muscle Response to Frequency of Stimulation a) Results in wave summation, incomplete tetanus, and fused (complete) tetanus Figure 9.13
c) Treppe: The Staircase Effect (figure 9.14) Muscular contractions become stronger with a repeated stimulus of the same strength, producing a stair case pattern on the myogram. This is the basis of the warm-up period required of athletes and is probably due to the increased availability of Calcium in the sarcoplasm and the liberation of contraction heat which makes enzymes (such as ATPase) more efficient.
c) Isotonic and Isometric Contractions Isotonic contractions occur when the muscle contracts and changes in length thereby decreasing the angle at the joint and moving the load. Once sufficient tension has developed to lift the load, the tension remains relatively constant through the rest of the contractile period. There are two types of isotonic contractions: 1) Concentric contractions are those in which the muscle shortens and does work picking up a book or kicking a ball 2) Eccentric contractions occur when the muscle contracts as it lengthens such as that which occurs in your calf muscles as you climb up a hill. Eccentric contractions are about 50% more forceful than concentric ones and more often delayed-onset muscle soreness occurs. The quadriceps muscles are stretched and contract (eccentrically) as your knees are flexed during deep knee bends which helps to protect your joints from injury. Isometric contractions occurs when the muscle neither shortens or lengthens. Isometric contractions occur when the muscle attempts to lift a load greater than the force that the muscle is able to develop.
4) Muscle Fiber Types Involved in Aerobic and Anaerobic Sports Activities a) Fast twitch fibers 1) appear white 2) They contract quickly in 0.01 seconds or less following stimulation 3) They are of larger diameter than other fibers 4) They have fewer mitochondria 5) They contain large glycogen reserves and produce powerful contractions and are used for quick bursts of speed for anaerobic exercise b) Slow twitch fibers 1) They contain pigment myoglobin which is used to store oxygen in reserve in resting muscle fibers 2) They contain many mitochondria 3) They appear red due to a very extensive network of capillaries which adds to their red appearance as they function extensively during aerobic exercise (exercises of endurance) 4) The fibers are thinner and weaker (a long distance runner may have more slow twitch fibers than a sprinter as one could see from comparing the size of their leg muscles) ***In chicken meat the legs have red meat (slow twitch fibers) while the breasts have white meat for endurance (flight). The same is true for the dark and white meat of turkey. We have both fast and slow twitch fibers each used for either anaerobic or aerobic activities.
COMPARISONS OF SKELETAL , CARDIAC, AND SMOOTH MUSCLE (TABLE 9.4)
NAMING SKELETAL MUSCLES Skeletal muscles are given names according to the following criteria: a) Location: Examples are the intercostals which run between the ribs and the temporalis overlies the temporal bone. b) Shape: An example would be the deltoid which is a roughly triangular muscle and the right and left trapezius form a trapezoid. c) Relative size: Examples include muscles named with terms such as maximus (largest), minimus (smallest), longus (long), and brevis (short). Gluteus maximus and the smaller gluteus minimus are specific examples. d) Direction of muscle fibers: Names such as rectus (straight) , transverse,and oblique describe the direction that the fibers run in reference to the midline of the body or the longitudinal axis of a limb or a bone. Examples include the rectus femoris ( straight muscle of the thigh, or femur), and the transverse abdominis (the transverse muscle of the abdomen). e) Number of origins: The terms biceps, triceps, quadriceps imply that the muscle has two,three, and four origins respectively. f) Location of the attachments: Muscles sometimes are named according to their points of origin and insertion in which the point of origin is named first. The sternocleidomastoid (a muscle of the neck) for example has two origins: one on the sternum (sterno), the other on the clavicle (cleido) and inserts on the mastoid bone. g) Action: Words such as flexor, extensor, or adductor are added to some muscles to describe their action. The supinator for example supinates the forearm while the adductor longus adducts the thigh.
ARRANGEMENT OF FASCICLES can determine the power of a muscle and how much a muscle can shorten. Types of fascicle arrangements include: a) Parallel arrangement includes muscles with fascicles that run parallel to the long axis of the body. They can be straplike like the sartorius, or spindle shaped with an expanded belly (midsection). The spindle shaped muscles are placed into a separate class known as fusiform muscles. The biceps brachii is an example of a fusiform muscle. b) Pennate arrangements include muscles which have short fascicles attaching obliquely to a central tendon that runs the length of the muscle. They are called unipenneate (extensor digitorum longus) if they insert into only one side of the muscle, bipennate (rectus femoris) if they insert from opposite sides of the tendon, and multipennate (the deltoid) if the arrangement looks like many feathers situated side by side (a combination of more than one bipennate arrangement attaching to the same tendon. c) Convergent muscles have a broad origin and its fascicles converge toward a single tendon of insertion. The muscle appears triangular or fan shaped. The pectoralis major muscle of the anterior thorax is an example. d) Circular arrangement occur when the fascicles are arranged in concentric rings. Muscles of this type surround external body openings which they close by contracting. Such muscles are called sphincters. Examples include the orbicularis oris of the mouth and eyes. ****Muscles with parallel fascicle arrangements provide the greatest degree of shortening, but are not very powerful. In contrast the more powerful muscles are the shorter stockier muscles that have the greatest number of fibers such as the bipennate and multipennate muscles. These muscles however cannot shorten as much as those with parallel fascicle arrangements.
LEVER SYSTEMS INVOLVING BONES AND MUSCLES Three types of lever systems include.... a) First-class levers are those in which the fulcrum is between the effort and the load. A pair of scissors, pliers, a bottle opener are mechanical examples. Raising your head off of your chest is an anatomical example. The joint (fulcrum) is the pivot point of fulcrum systems in the body. In this case the joint between the atlas and the occipital condyles is the fulcrum, while the load represents the anterior portion of the head and the effort is being supplied by the posterior neck muscles. The mechanical advantage of this type of lever will vary as the distance changes between the fulcrum and the load to be lifted. The closer the fulcrum is to the load the greater the mechanical advantage (as lifting your head as described above) , but it results in less movement. The further the fulcrum is away from load then the less the mechanical advantage, but there is an increase in the range and speed of movement. (action of the triceps muscle in extending the forearm). b) Second-class levers are those in which the load is between the fulcrum and the effort. A mechanical example would be lifting a wheelbarrow. In our bodies standing on our toes would be an example (the calf muscles producing the effort). Second-class levers are uncommon in the body. c) Third-class levers are those in which the effort applied is between the load and and the fulcrum. Mechanical examples are lifting a shovel full of soil, sweeping with a broom, and a pair of forceps. In our bodies the flexion of our forearm by the biceps brachii is an example of a third class lever. ***Systems that operate at a mechanical advantage ( requiring less force to lift a larger load) are slower, more stable and used where strength is a priority. Systems that do not operate at a mechanical advantage (a mechanical disadvantage) are speed levers, force is lost but speed and range of movement are gained. MAJOR SKELETAL MUSCLES OF THE BODY Muscles of the Head, Part 1: Facial Expression (Figure 10.6) a) include muscles of the scalp and face b) adjacent muscles seem to be fused c) unusual in that they insert into the skin, other muscles, but not bones d) The main muscle of the scalp is the epicranius consisting of the frontalis and the occipitalis. The frontalis has as its point of origin the gala aponeurotica(a cranial aponeurosis- an aponeurosis which is a fibrous or membraneous sheet that connects a muscle and the part it moves) and the occipitalis inserts on the gala aponeurotica. e) Actions of the scalp and face lift the eyebrows, flare the nostrils, open and close the eyes and mouth, and the smile. f) All muscles of the face are innervated by cranial nerve VII (the facial nerve). Paralysis of these muscles are apparent because of the loss of nonverbal communication after a stroke. (table 10.1 and figure 10.6)
Muscles of the Head, part 2: Mastication and Tongue Movement (Figure 10.7) a) Four pairs of muscles are involved in chewing and biting actvities (mastication) all innervated by the mandibular division of cranial nerve V (the trigeminal nerve): the masseter and the temporalis muscles (prime movers of jaw closure), the medial and lateral pterygoid muscles ( perform grinding movements), the buccinator muscles (helps to keep food between the grinding surfaces of the teeth). Neck muscles such as the digastric and mylohoid muscles can depress the mandible if there is resistance to jaw opening (normally gravity is sufficient to depress the mandible). b) Only muscles of the tongue that serve to anchor and move the tongue called extrinsic tongue muscles (table 10.2 ; figure 10.7) are considered here. Intrinsic tongue muscles that curl, squeeze, and fold the tongue during speaking and chewing are studied with the digestive system. Muscles of the Anterior Neck and Throat: Swallowing (Figure 10.8) a) Consists of the suprahyoid and infrahyoid muscles of the anterior neck. The neck is divided into two triangles (anterior and posterior) by the sternocleidomastoid muscle. The anterior traiangle or anterior neck muscles are used in the swallowing process (table 10.3; figure10.8) Muscles of the Neck and Vertebral Column: Head and Trunk Movements (Figure 10.9) a) The major head flexors are the sternocleidomastoid muscles which are often called the "prayer muscles" (the supra hyoid and infrahyoid muscles act as synergists in this movement). The sternocleidomastoids also act in lateral head movements along with the deeper muscles called the scalenes along with several straplike muscles at the back of the neck. b) Head extension is accomplished mostly by the splenius muscles, but is aided by the more superficial trapezius muscle of the back. c) Trunk extension is served by the intrinsic back muscles which also aide in maintaining the normal curvature of the spine. They have their points of origin and insertion on vertebrate,the iliac crests, occipital and temporal bones of the skull ( table 10.4; figure 10.9). Muscles of the Thorax: Breathing (Figure 10.10 a) The diaphragm is the prime mover of inspiration divides the thoracic from the abdominopelvic cavities. When it is relaxed it is dome shaped, but when it contracts it moves inferiorly and flattens increasing the volume of the thoracic cavity causing air to rush into the lungs. Pressure changes occur below the diaphragm due to its alternating contraction and relaxation that facilitates the return of blood to the heart. The diaphragm can also be contracted voluntarily to push down on the abdominal viscera increasing the pressure in the abdominal cavity to help evacuate urine, feces, or a baby and during weight lifting. b) The external intercostal muscles between the ribs are the synergists of the diaphragm (aiding the diaphragm in the process of inspiration. They lift the rib cage increasing the dimensions of the thorax causing air to rush into the lungs. c) The internal intercostal muscles lie deep to the external intercostals between the ribs and upon contraction will cause a "forced" expiration of air from the lungs. Quiet respiration is passive resulting from the relaxation of the external intercostals and diaphragm along with the elastic recoil of the lungs. The muscle fibers of both of the intercostal muscles run obliquely and at right angles to one another. Muscles of the Abdominal Wall: Trunk Movements and Compression of Abdominal Viscera (Figure 10.11) a) Four pairs of muscles are found in the abdominal wall. The lateral abdominal walls are formed from the following three pairs of muscles from the most superficial to the deepest: the external oblique, the internal oblique and the transverse abdominis. The fibers or fascicle directions alternate with each other much like the construction of plywood in which the grains of the wood runs at right angles. This type of arrangement in the abdominal muscles provide added strength to the abdominal wall which have no bony reinforcements (ribs) to protect them as in the thorax. These muscles blend together anteriorly and insert onto an aponeuroses anteriorly. The aponeuroses incloses a fourth muscle pair called the rectus abdominis muscles which fuse together forming the linea alba a tendinous seam running the length from the sternum to the pubic symphysis. Enclosing the rectus abdominis within the aponeuroses stabilizes them preventing the rectus abominis muscles from protruding anteriorly. b) The abdominal muscles protect and support the viscera best when they are well toned. When weak or severely stretched as in a pregnancy they can result in a potbelly (abdomen becomes pendulous or like a pendulum-swinging back and forth). The contraction of these muscles along with the diaphragm causes the glottis to close and causing an increase in intra-abdominal pressure to help promote urination, defecation, childbirth, vomiting, coughing, screaming, sneezing, burping and nose blowing. Your abdominal muscles can be felt contracting under the skin during each of these activities. During heavy weight lifting these muscles also can contract sometimes so forcefully that hernias can result. Muscles of the Pelvic Floor and Perineum: Support of Abdominopelvic Organs (Figure 10.12) a) The pelvic floor (pelvic diapharagm) is formed from two paired muscles the levator ani and the coccygeus. These muscles act to 1) close the inferior outlet of the pelvis 2) support the pelvic floor and elevate it to help release feces and 3) to resist increased intra-abdominal pressure which would expel the contents of the bladder and the uterus. b) The pelvic diaphragm is pierced by the rectum, urethra, and the vagina (in females). The body region inferior to the pelvic diaphragm is the perineum. The urogenital diaphragm forms the anterior half of the perineum. The urogenital diaphragm consists of a trangular sheet of muscle containing the sphincter urethrae which surrounds the urethra and allows voluntary control of urination. Superficial to the urogenital diaphragm and covered by the skin of the perineum is the superficial space which contains the muscles that help erect the penis and the clitoris (ischiocavernosus and the bulbospongiosus). In the posterior half of the perineum lies the external anal sphincter encircling the anus and allows voluntary control of defecation. Anterior to the anal spincters is the central tendon of the perineum a strong tendon into which many of the perineal muscles insert. Superficial Muscles of the Anterior and Posterior Thorax: Movements of the Scapula (Figure 10.13 a) The superficial muscles are called extrinsic muscles, run from the ribs and vertebral column to the shoulder girdle and act to fix the scapula to the wall of the thorax or move the scapula to effect arm movements. They are divided into the anterior and posterior thorax muscles b) Muscles of the anterior thorax include the pectoralis major, pectoralis minor, serratus anterior, and subclavius. All of the these muscles insert into the pectoral girdle except for the pectoralis major which inserts into the humerus. c) Muscles of the posterior thorax include superficially the latissimus dorsi and the trapezius muscles and the underlying levator scapulae and the rhomboids. The latissimus dorsi inserts into the humerus like the pectoralis major and is more concerned with movements of the arm rather than the scapula. d) The prime movers of shoulder elevation are the trapezius and the levator scapulae. When acting together their opposite rotational effects counterbalance each other resulting in a "shoulder shrug". e) The scapula is depressed largely by the weight of the arm due to gravity, and depressed further by the trapezius, serratus anterior and the latissimus dorsi. f) Forward movements (abduction) of the scapula as in pushing or punching movements involve the serratus anterior. g) Retraction (adduction) of the scapula involves the trapezius and the rhomboids. The serratus anterior and the trapezius muscles act together to coordinate rotational movements of the scapula and are antagonists in forward or backward movements of the scapula. Muscles Crossing the Shoulder Joint: Movements of the Arm(figure 10.14 a) All muscles crossing the shoulder joint insert on the humerus and originate from the pectoral girdle. The latissimus dorsi and pectoralis major however also originate on the axial skeleton. There are nine muscles crossing each shoulder joint. b) The prime movers of the nine muscles include the superficial pectoralis major, latissimus dorsi, and the deltoid muscles. The remaining six muscles are synergists and fixators. Four of these six are called rotator cuff muscles: supraspinatus, infraspinatus, teres minor, and the subscapularis. They originate on the scapula, and their tendons blend with the fibrous capsule joint of the shoulder on their way to the humerus. The main function of the rotator cuff muscles is to reinforce the capsule of the shoulder joint to prevent dislocation of the humerus (ball and socket joints are the most flexible joints in our body and also the most instable), but they also act as synergists in the angular and rotational movements of the arm. The remaining two muscles are the teres major (synergist of the latissimus dorsi) and the coracobrachialis (synergist of the pectoralis minor) which cross the shoulder joint, but do not help in reinforcement. Muscles Crossing the Elbow Joint: Flexion and Extension of the Forearm(figure 10.14) a) These muscles act to flex and extend the forearm and are divided by walls of fascia into two muscle compartments: the posterior extensors and the anterior flexors. b) The posterior compartment contains triceps brachii which is the prime mover of forearm extension and is assisted by the anconeus muscle (a synergist). c) The anterior compartment which causes elbow flexion consists of (in order of decreasing strength) the brachialis, the biceps brachii, and the brachioradialis. The brachialis and biceps are inserted into the ulna and radius respectively and contract simultaneouly during flexion. The biceps muscle also supinates the forearm and is ineffective in flexing the elbow when the forearm must stay pronated (it is harder to to chinups when your palms are facing away from your body). Muscles of the Forearm : Movements of the Wrist, Hand and Fingers (Figures 10.15 and 10.16) a) The forearm muscles are divided into two main compartments by fascia: the anterior flexors and the posterior extensors, each having superficial and deep layers. Functionally the forearm muscles cause either movements of the wrist, or movement of the fingers and thumb. Strong ligaments called the flexor and extensor retinacula or "wrist bands" keep the tendons from jumping outward when tensed. b) Most of the anterior forearm muscles are wrist or finger flexors two muscles are pronators: the pronator teres, and the pronator quadratus. Pronation is one of the most important forearm movements. c) Muscles of the posterior compartment extend the wrist and fingers. An exception to this is the supinator muscle which assists the biceps brachii muscle of the arm in supinating the forearm. Intrinsic Muscles of the Hand: Fine Movements of the Fingers (Figure 10.18) a) These include the main abductors and adductors of the fingers as well as muscles that produce the movement of opposition (opposing thumb movement). All move the metacarpals and fingers and are located in the palm (none on the dorsal surface of the hand). They control the precise movements such as threading a needle while the forearm muscles control the "power grip" of our hand. b) The intrinsic muscles of the palm are divided into three groups: 1) the thenar eminence (ball of the thumb) 2) the hypothenar eminence (ball of the little finger) 3) the midpalm. The thenar and the hypothenar each contain a small flexor, and abductor, and an opponens muscles while the midpalmer muscles contain the lumbricals and the interossei which extend our fingers at the interphalangeal joints. The interossei are also the main finger abductors and adductors. Muscles Crossing the Hip and Knee Joints: Movements of the Thigh and Leg (Figures 10.19 and 10.20) a) The muscles in the thigh are separated by walls of fascia into anterior, posterior and medial comparments. The deep fascia of the thigh called the fascia lata surrounds and encloses all three groups of muscle. The muscles in the anterior compartment act to flex the femur at the hip and extend the leg at the knee (the foreswing phase of walking). The muscles in the posterior compartment extend the thigh and flex the leg (the backswing of walking). The muscles in the medial compartment are the medial or adductor muscles and all adduct the thigh, having no effect on the leg. b) The thigh (femur) flexors pass in front of the hip joint and include the iliopsoas, tensor fasciae latae, and the rectus femoris. They are assisted by the adductor muscles of the medial thigh and the sartorius. The prime mover of thigh flexion is the iliopsoas. c) Thigh extension is accomplished by the hamstring muscles (the biceps femoris, the semitendinosus, and the semimembraneous). and during forceful extension by the gluteus maximus which are the buttocks muscles which lie lateral to the hip joint. The gluteus maximus consist of the gluteus medius and minimus which also act to abduct the thigh and rotate it medially. The gluteus maximus is most effective when force is necessary as in rising from a forward flexed position (forward thrusts), or in thrusting the thigh posteriorly in climbing the stairs and running which produce "buns of steel" (generally inactive in standing and walking). d) The sole knee extensor is the quadriceps femoris the muscle of the anterior thigh and the most powerful muscle of the body. The quadriceps include four heads : the rectus femoris, the vastus lateralis, the vastus medialis, and the vastus intermediaus. All four heads have a common insertion tendon called the quadriceps tendon which inserts into the patella. The quadriceps is a powerful knee extendor used in climbing, running, jumping, and rising from the seated position. The quadriceps is antagonized by the hamstrings which are the prime movers of knee flexion. Muscles of the Leg: Movements of the Ankle and Toes (Figures 10.21 to 10.23) a) The leg muscles are separated into the anterior, lateral, and posterior compartments by the inward extension of the fascia lata which is continuous with the fascia lata which encloses the thigh. The fascia lata binds the leg muscles tightly helping to prevent swelling during exercise and to also aid in venuous return of blood. Distally the leg fascia thickens to form the flexor, extensor, and fibular (or peroneal) retinaculae, which secure the muscle tendons in place as they cross the ankle to run to the foot. b) Muscles in the anterior extensor compartment include the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and they which are primarily toe extensors and ankle dorsiflexors. Dorsoflexion is not a powerful movement, but is important in keeping the toes from dragging when walking. c) Lateral compartment muscles include the fibular or peroneal muscles that plantar flex and evert the foot. d) Muscles of the posterior flexor compartment include the gastrocnemius, soleus, tibialis posterior, flexor digitorum longus, and the flexor hallucis longis. These muscles act to planter flex the foot and to flex the toes. Plantar flexion is the most powerful movement of the ankle and the foot because it lifts the entire weight of the body. It is essential for standing on tiptoe and providing the necessary forward thrust while walking and running. The popliteus muscles is important in "unlocking" the knee in preparation for flexion. Intrinsic Muscles of the Foot: Toe Movement and Arch Support (Figure 10.25) a) These muscles help to flex, extend, abduct, and adduct the toes. There is a single muscle on the dorsum of the foot (superior aspect) called the extensor digitorum brevis and several muscles on the plantar surface (the sole) which occurs in three layers as as listed in table 10.17.
|
|
|