

Dr Arun Prasad, MBBS (AFMC), MS (New Delhi), FRCS (Edin) & FRCS (Glas)
Senior Consultant, Minimal Access Surgery, Apollo Hospital, New Delhi
Laparoscopic hernia repair is rapidly gaining popularity in the West and in India despite early criticism of the futility of this procedure. Open hernia repair is being done for centuries with 'excellent' results then why complicate issues with this new technique. Most surgeons would agree that Laparoscopic removal of gall bladder is now the best way of treating gall stones and gall bladder disease but for hernia repair, they still have their reservations.
A hernia commonly occurs in the groin when the fat and intestines from the tummy force their way out of a defect in the muscle. Bulging out of tummy contents through this causes pain and there is a danger of the intestine to get strangulated. The problem increases with time and unfortunately the only treatment for this condition is surgery. This traditionally involved a cut over the hernia, reduction of the contents back to the tummy and some form of stitching of the defect to prevent the hernia from coming back.
The main problem with a hernia operation is the average six weeks of rest after surgery and the chance of the hernia coming back ( failed operation that is known in medical terms as a recurrent hernia). Many proud surgeons would say that their patients don't get recurrent hernias but studies abroad have shown that the patient with recurrent hernia seldom goes to the same surgeon. Also the large number of operations being done for recurrent hernia confirms this study. Detailed statistical analysis revealed that the recurrence rate is about 20%. This prompted the Royal College of Surgeons of England to issue guidelines for surgeons. The best international results were by a technique known as Liechtenstein repair that showed a recurrence of less than 1%. What was good about this technique is that even average surgeons who are not specialised in hernia surgery, produced the same good results. The techniques basically involve minimum stitching and a tensionless placement of a net (mesh) at the defect site with little disturbance to the body physiology. However all open surgical techniques involve cutting of the muscles overlying the hernia in order to be able to reach the defect. Which in effect weakens already weak muscle tissue. This like any other way of hernia repair means pain and rest after the operation.
THE PRINCIPLE OF LAPAROSCOPIC HERNIA REPAIR
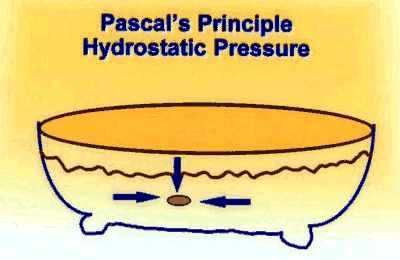 Imagine a bathtub. When you put the rubber stopper at the outlet and fill it with water, the water pressure pushes the stopper in place and keeps it fixed there. The more the water, the firmer is the stopper. Now, if we were to put the stopper from the outside. Then the water pressure in the tub is going to push the stopper out as the pressure increases. This is Pascal's law.
Imagine a bathtub. When you put the rubber stopper at the outlet and fill it with water, the water pressure pushes the stopper in place and keeps it fixed there. The more the water, the firmer is the stopper. Now, if we were to put the stopper from the outside. Then the water pressure in the tub is going to push the stopper out as the pressure increases. This is Pascal's law.
The same scenario can be imagined with placing a mesh on the hole where the hernia is. Is it going to be better fixed from outside or inside? Open surgery places it from outside and laparoscopic surgery places it from inside as is shown in the photographs below.
1. Fat being pulled in from the hernial defect, 2. The defect as it looks from the inside,



During laparoscopic surgery, we make a small ½ inch cut in the skin at the belly button. Then a cannula (thin tube) is introduced in between the muscle fibres without cutting any of the muscle. Through the cannula, the laparoscope is inserted into the patient's body. It is equipped with a tiny camera and light source that allows it to send images through a fibre-optic cord to a television monitor. The television monitor shows a high resolution magnified image. Watching the monitor, the surgeon can perform the procedure. While looking inside the patient, further two ½" diameter cannulas are put in. This way, the already weak muscles are not disturbed and the net is placed through the half inch holes that are away from the hernia. Thus there is minimal disturbance to the normal body physiology and as a result the pain is minimal and very little rest is required. Also the hernia that is going out from the tummy is pulled back in rather than pushed in from outside as is done in an 'open' operation. There are more and more reports now from the USA and Europe showing the success of this technique in reducing post operative pain, rest and recurrence rates.
Click below to see video of Dr Arun Prasad doing Laparoscopic Hernia Surgery.
The greatest advantage of laparoscopic surgery for hernias is in patients of recurrent hernias where the anatomy has already been disturbed and also in patients of hernias on both sides, as they can be repaired through the same three holes avoiding any further pain or trauma.
The two real problems of the laparoscopic hernia repair are the cost of the operation, due to the expensive imported instruments that are needed ; and the necessity for general anaesthesia. The increased cost should be compared with the gain associated by a quicker and more productive return to work by the majority of the patients.
Laparoscopic hernia is an efficient technique that compares favourably to current open surgical techniques. Patients are relatively pain free following this procedure and can return to work and normal activities much quicker than following conventional hernia repairs. Recent reports from the USA show that these patients took an average of 9 days off work compared to 48 days after an open operation.
MAJOR RECOMMENDATIONS OF NATIONAL INSTITUTE OF CLINICAL EXCELLENCE ( NICE ), LONDON, UK
Laparoscopic surgery is recommended as one of the treatment options for the repair of inguinal hernia. To enable patients to choose between open and laparoscopic surgery (either by the transabdominal preperitoneal [TAPP] or by the totally extraperitoneal [TEP] procedure), they should be fully informed of all of the risks (for example, immediate serious complications, postoperative pain/numbness, and long-term recurrence rates) and benefits associated with each of the three procedures. In particular, the following points should be considered in discussions between the patient and the surgeon: The individual's suitability for general anaesthesia The nature of the presenting hernia (that is, primary repair, recurrent hernia, or bilateral hernia) The suitability of the particular hernia for a laparoscopic or an open approach The experience of the surgeon in the three techniques Laparoscopic surgery for inguinal hernia repair by TAPP or TEP should only be performed by appropriately trained surgeons who regularly carry out the procedure.
Read the full text of the above by clicking here.
Common Questions asked
Q. What are the main advantages ?
A. There is no cutting of muscles hence minimal pain and early return to normal activity. Secondly, as the mesh is placed from inside covering the defect in a very secure way, the chances of the hernia coming back is extremely low.
Q. What is the recovery period?
A. The patient can start drinking liquids soon after coming out of the anaesthesia which is about 4 hours after the operation. They can start eating soon thereafter. The patient is allowed to get off the bed 4 hours after the surgery and walk to the toilet to pass urine. They are usually allowed to go home the next day, can climb stairs and the majority can get back to routine activity in 5 days and back to work in about 10 days.
Q. What are the chances of the hernia coming back?
A. Almost nil if the operation has been done properly as has been shown in numerous studies abroad.
Q. Is it more risky for patients with other medical problems like diabetes and blood pressure?
A. No. On the contrary, the absence of any major cuts to the body causes minimal disturbance to the physiology. Also the early mobility and return to normal diet makes it easy for the body to recover.
Q. Is their any danger from the telescope inside the body?
A. No, the telescope is used only to see and is not involved with the operation.
Q. Is their an increased risk of infection?
A. No, the small cuts mean that less of the body is exposed to infection.
Q. Why do you approach the hernia from inside?
A. The hernia is protrusion of the body contents through the weakness in the muscle. It is logical that something coming from inside is best dealt from inside. Also this way one does not cut and weaken the already weak muscles at the hernia site.
Q. How safe is it to leave a mesh inside the body?
A. The mesh used is the same as the one used for open operations over last 30 years. Its safety and efficacy is beyond doubt as proved by the numerous trials in the USA and Europe.
Q. Is this all very expensive? How can one justify the cost of the equipment and surgery in a country like India?
A. The cost of laparoscopic equipment and the ' one use only (disposable) ' instrument that is used to fix the mesh inside increases the cost of surgery. Unfortunately these are still imported and will remain expensive till thy are locally produced. However, the increased cost should be compared with the gain associated by a quicker and more productive return to work by the majority of the patients. The hidden lowering of cost is due to less leave, early return to normal activity and work, and also from the greatly reduced disruption of the family rou-tine.
Q. Any advantage to the Indian situation as compared to the West?
A. In the west, the support systems are much better. Most patients travel by car or by public transport which is user friendly like having steps reaching down to the road, ramps and escalators at railway stations and subways. Most people can afford a rest after surgery. In India, the situation is quite the reverse. Buses have high steps and usually it is a fight or atleast a struggle to get on to the bus which can move any time without any warning. There are no ramps in most railway stations or subways. All systems require straining if someone who has had surgery has to go out. Scooters and cycle rides are not possible without straining. Most people are self employed and cannot afford prolonged rests. Hence minimally invasive treatment like laparoscopy for hernia is more appropriate for countries like ours than to the US and Europe.
The author Dr Arun Prasad MS, FRCS, FRCSEd is a Senior Consultant Laparoscopic Surgeon at Apollo Hospital, New Delhi.
Also a teacher in Laparoscopic Surgery at Ethicon Institute of Surgical Education, Mumbai & New Delhi and Tutor for the Royal College of Surgeons, UK.
He was a surgeon at Charing Cross Hospital and Medical School, London and a teacher in Laparoscopic Surgery at The Royal College of Surgeons, London.
He is one of the few trained Laparoscopic surgeons doing hernia repair and is a world pioneer in this technique.
