
An abdominal aortic aneurysm (AAA) represents a localized dilation of the largest blood vessel in the lower part of the body, which supplies blood to the legs. With the increasing age of the population, the incidence of AAA rises sharply. The incidence of AAA is approximately 50 to 55 per 100,000 per year in men aged 55 to 64 years and nearly ten times that number in men over 80 years.
Anatomy and Pathology
The aorta is the largest blood vessel in the body. It begins at the heart and passes backward to be located deep in the body just in front of the bony spine. When it passes through an opening in the diaphragm it becomes the abdominal aorta. As the aorta passes into the pelvis it splits into the common iliac arteries. The most important branches of the abdominal aorta feed the kidneys and bowel. (Figure 1).
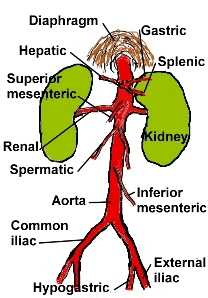 |
| Figure 1 - Anatomy showing the abdominal aorta and its branches. The abdominal aorta extends from the diaphragm to the iliac vessels. The branches feed the organs within the abdominal cavity. |
The frequency of aneurysms to form in this location relates to abnormalities in blood flow as well as changes which occur to the blood vessel wall over time due to hardening of the arteries (atherosclerosis). The aneurysm wall may contain calcium deposits. And small blood clots (thrombi) may form on the wall. In general, aneurysms expand over time and ultimately burst, much like a balloon which continues to expand and finally bursts. When an aneurysm ruptures, there are often catastrophic consequences
These sobering facts point out the lethal nature of AAA and would seemingly strongly favor surgery for any AAA. However, It appears that small aneurysms (less than 4 cm. or 1.6 inches) seldom rupture at the same rate as do larger ones. When the aneurysm reaches around 5 cm (2 inches) there is a sharp increase in aneurysm rupture. Therefore most vascular surgeons do not recommend elective repair for aneurysms smaller than 4 cm.
History and Examination
Occasionally they produce some vague back pain or abdominal throbbing
In contrast, an AAA that has ruptured causes
Rupture of an AAA is an urgent surgical emergency with mortality rates of 50 to 70%
Special Tests
Noninvasive tests
Abdominal Ultrasound. An ultrasonic sensor connected to a special computer and monitor is placed over the abdomen. This produces a picture of the abdominal contents and is an accurate method for measuring the size of an AAA. Ultrasound is commonly used to follow patients with aneurysms less than 4 cm in diameter. It provides an excellent method for assessing aneurysm growth over time. Once an aneurysm reaches the 5 cm, elective surgical repair is necessary (Figure 2).
 |
| Figure 2 - Abdominal ultrasound of a 6.5 cm. (2.6 inches) abdominal aortic aneurysm. The small arrows outline the aneurysm wall. Blood flow through the lumen is in color while clot lies between the wall and lumen (Courtesy S. Sadiq, M.D.) |
 |
| Figure 3 - CT scan through an 8.5 cm. (3.4 inches) abdominal aortic aneurysm. Note the clot that fills most of the aneurysm. The lumen is open and is where the blood flows. Courtesy S. Sadiq, M.D. |
Invasive testing utilizes a special catheter placed in the artery under fluoroscopic control. A dye that shows up on X-ray is injected through the catheter. Serial X-ray films or aortogram are then obtained of the aorta. This produces the most accurate picture of the aneurysm. For routine AAA below the level of the arteries to the kidneys, a CT scan provides enough information to make arteriogram unnecessary (Figure 4).
 |
| Figure 4 - Aortogram of an abdominal aortic aneurysm. Note small linear calcifications in the wall of the aneurysm (multiple small arrows) and the clot (*) between wall and lumen. Courtesy S. Sadiq, M.D. |
Surgical Treatment
Elective repair provides an excellent option for those individuals who have an AAA 5 cm or greater
Therefore the overall risks associated with an elective repair is between 5-8% versus 60-75% risk of dying with emergent repair of a ruptured AAA. AAAs between 4 and 5 cm represent a group of patients whose management remains controversial. Some of the factors that increase the likelihood of AAA growth are:
Other considerations before carrying out surgery are
Surgical Procedure
 |  |
| 5A - AAA extending from just below the renal arteries to the iliac arteries. | 5B - Vascular clamps are placed across the aorta below the renal arteries and across the common iliac arteries. The aneurysm is opened. |
 |  |
| 5C - The clot that lines the inner wall is removed. The wall of the aneurysm is preserved. | 5D - The graft is sutured in place between the upper and lower ends of the aorta. |
 | |
| 5E - The preserved wall of the aneurysm is wrapped around the graft and following which the clamps are removes to allow blood to flow through the graft. |
Complications
Post Operative Care
